For Retinal Physician's Surgical Pearls video series, Melissa Yuan, MD, and Ehsan Rahimy, MD, demonstrate induction of a posterior vitreous detachment in a young, phakic patient. Transcript of the narration follows below:
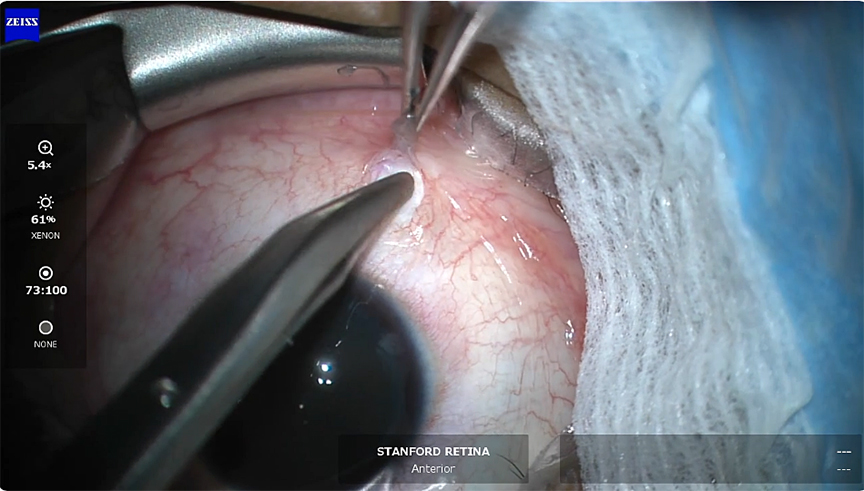
This is Melissa Yuan, retina fellow at Stanford, in conjunction with Dr. Ehsan Rahimy, a retina specialist at Palo Alto Medical Foundation and Stanford. This video demonstrates induction of a posterior vitreous detachment in a young, phakic patient.
This patient had visually significant floaters that were significantly impacting their quality of life. Despite phakic status and no preexisting posterior vitreous detachment and a lengthy discussion of risks and benefits, the patient elected to proceed with vitrectomy.
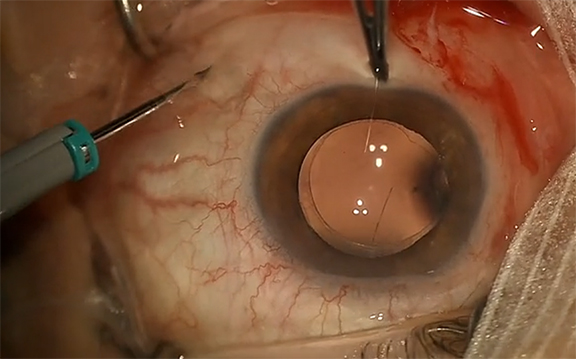
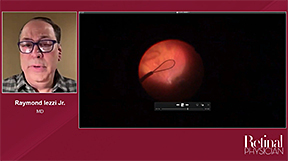
The floater is visible here after trocar placement.
A core vitrectomy is performed, and the ports are cleared.
Kenalog is instilled to assist with visualization.
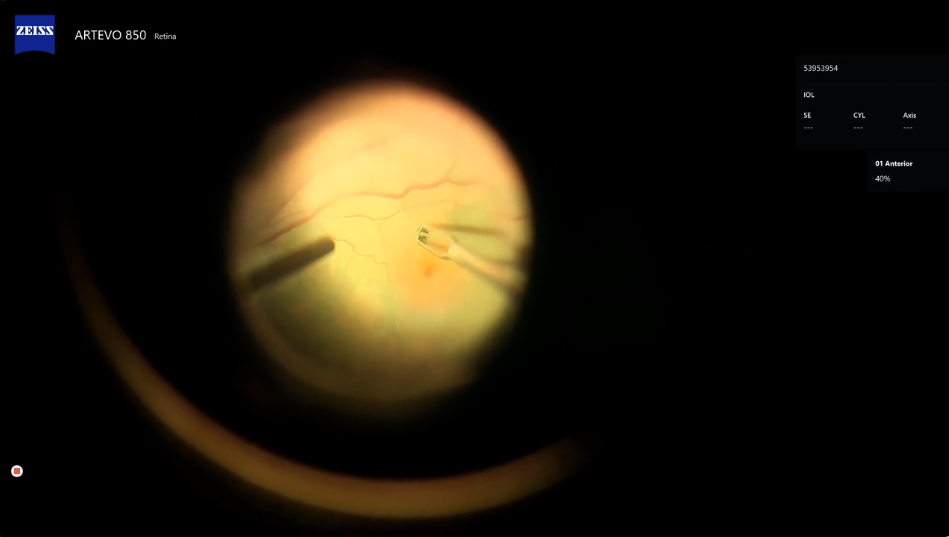
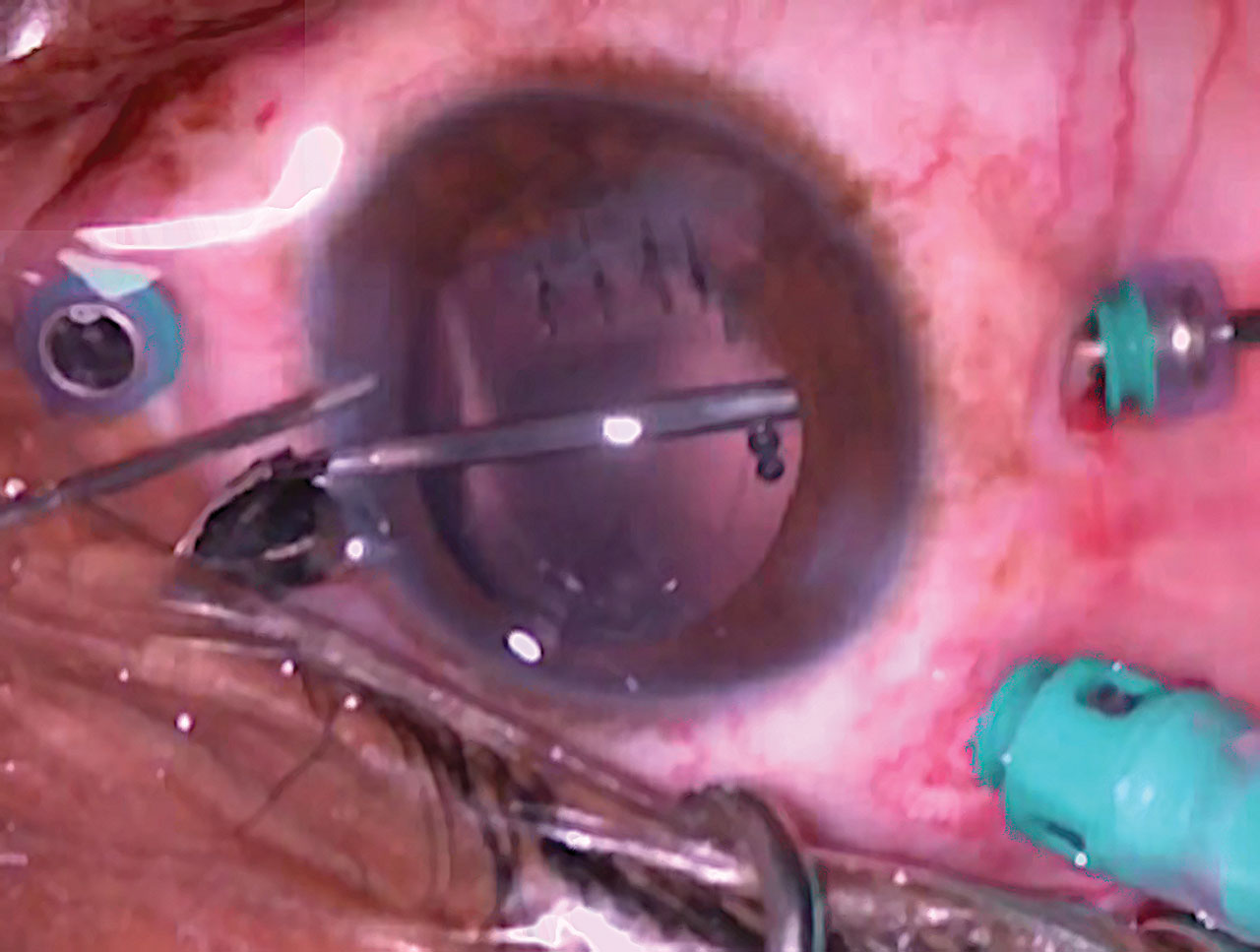
We then turn our attention to inducing a posterior vitreous detachment. The cutter mode is turned off and we are on aspiration only. The vitrector port is positioned facing to the side over the optic disc. Aspiration at maximal vacuum of 650 mmHg is begun in order to engage the strands of vitreous. When the vitreous has been engaged, the vitrector is lifted tangentially and away from the retina, with care not to damage the lens and while watching the leading edge of posterior hyaloid elevation for tears. Several attempts are made to lift the hyaloid, which is quite adherent in this young patient. With each attempt, an effort is made to engage the vitreous in the area where there is some elevation or an opening in the posterior hyaloid.
Here, we successfully elevate the posterior hyaloid to the midperiphery.
After the posterior hyaloid has been successfully elevated, we switch back to cutting and complete the vitrectomy. RP


Other Videos From Series