







Michael A. Singer, MD: For this month’s Retina Minute, I have the pleasure of interviewing Jordana G. Fein, MD, who practices at the Retina Group of Washington and serves on the faculty at Georgetown University School of Medicine in Washington, DC. Dr. Fein, you recently presented the 64-week data from the QUASAR study evaluating aflibercept 8 mg (Eylea HD; Regeneron) for retinal vein occlusion (RVO). Can you explain what the study was about and how it was designed?
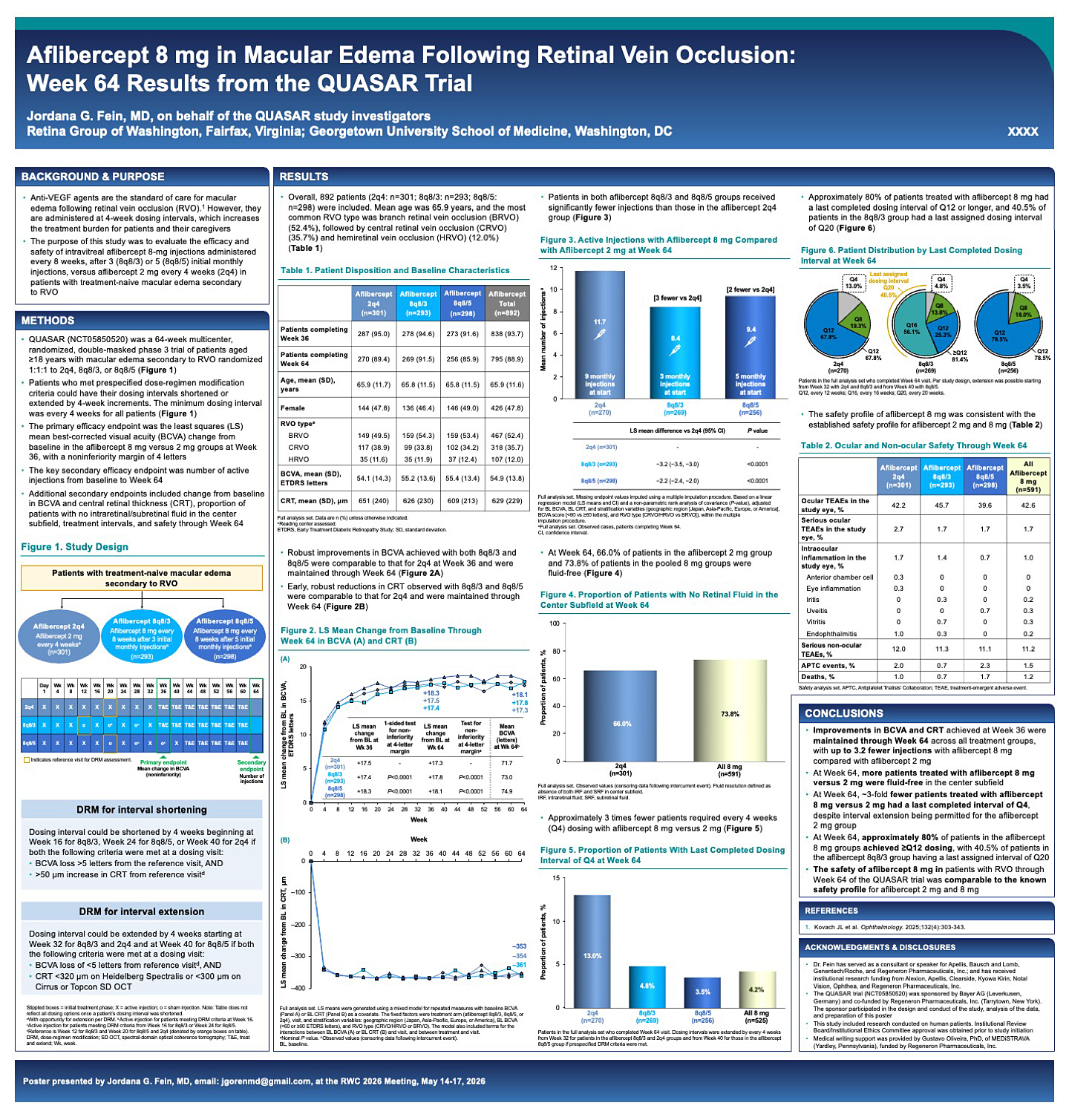
Figure 1. Improvements in BCVA and CRT achieved at Week 36 were maintained through Week 64 across all treatment groups, with up to 3.2 fewer injections with aflibercept 8 mg compared with aflibercept 2 mg.
Jordana G. Fein, MD: Absolutely. QUASAR was a 64-week, multicenter, randomized, double-masked phase 3 trial that enrolled treatment-naive patients aged 18 years and older with macular edema secondary to RVO.
Patients were randomized 1:1:1 to receive aflibercept 2 mg (Eylea; Regeneron) every 4 weeks, or aflibercept 8 mg every 8 weeks following either 3 or 5 monthly loading doses. Essentially, the study compared extended 8-week dosing intervals with standard monthly dosing.
Patients who met prespecified criteria could have their dosing intervals shortened or extended in 4-week increments, with a minimum dosing interval of 4 weeks. The primary efficacy endpoint was at week 36 and assessed noninferiority of aflibercept 8 mg compared with aflibercept 2 mg. Key secondary endpoints included the number of injections through week 64, as well as changes in BCVA, central subfield thickness (CST), absence of intraretinal or subretinal fluid in the central subfield, treatment intervals, and safety outcomes.
Dr. Singer: What did the results show?
Dr. Fein: First and foremost, QUASAR met its primary endpoint. At week 36, aflibercept 8 mg was noninferior to aflibercept 2 mg with respect to visual acuity and anatomic outcomes (Figure 1).
What is particularly interesting about the 64-week data is that it provides an early look at durability. By week 64, patients in the 2-mg arm received a mean of 11.7 injections. In comparison, patients in the aflibercept 8-mg groups received between 8.4 and 9.4 injections, depending on whether they received 3 or 5 loading doses. That translates to approximately 2 to 3 fewer injections over the study period, which was statistically significant.
Dr. Singer: Can you review the criteria for interval shortening and extension?
Dr. Fein: Certainly. Interval shortening could begin at week 16 in the 8-mg group that received 3 loading doses and at week 24 in the 8-mg group that received 5 loading doses. In the 2-mg arm, interval shortening could begin at week 40. To qualify for interval shortening, patients had to lose at least 5 letters of BCVA and demonstrate at least a 50-µm increase in CST compared with the reference visit.
Interval extension was also performed in 4-week increments. Patients could begin extending at week 32 in the 3-loading-dose group and at week 40 in the 5-loading-dose group. To qualify, BCVA loss had to be less than 5 letters, and CST had to remain below 320 µm on Heidelberg OCT or below 300 µm on Cirrus or Topcon OCT.
One point worth emphasizing is that because the primary endpoint occurred at week 36, patients had only recently begun extending treatment intervals. The 64-week data therefore represent just the beginning of what we may learn about long-term durability.
Dr. Singer: What percentage of patients were able to reach 12- and 16-week intervals?
Dr. Fein: In the 8-mg group that received 3 loading doses, 81.4% of patients achieved treatment intervals of at least 12 weeks, and 56% reached intervals of at least 16 weeks. In the 8-mg group that received 5 loading doses, 78.5% achieved intervals of at least 12 weeks. Only about 14% to 18% of patients in the 8-mg groups required every-8-week dosing at week 64, and just 3.5% to 5% required every-4-week dosing.
By comparison, in the 2-mg group, 67.8% reached 12-week intervals, 19% remained on every-8-week dosing, and 13% required every-4-week dosing.
Dr. Singer: How were interval adjustments made?
Dr. Fein: Both interval extension and shortening were performed in 4-week increments. That may differ somewhat from real-world practice, where adjustments are often made in smaller increments, but it was the protocol used in the study.
Dr. Singer: Were there any safety concerns associated with the 8-mg dose?
Dr. Fein: No new safety signals were identified. Rates of ocular adverse events, serious ocular adverse events, serious nonocular adverse events, Antiplatelet Trialists' Collaboration events, and deaths were balanced across treatment groups.
The rate of intraocular inflammation was 1.7% in the 2-mg arm and 1.0% in the 8-mg arm, so there was no indication of increased inflammation with the higher dose.
Another important finding relates to retinal fluid. At week 64, approximately 66% of patients in the 2-mg arm were free of retinal fluid in the central subfield, compared with approximately 74% of patients in the 8-mg groups. This suggests improved drying with aflibercept 8 mg.
Dr. Singer: How does this influence your approach to treating patients with RVO?
Dr. Fein: In my practice, I typically treat monthly initially and begin extending once the macula is dry. I generally extend more cautiously than the protocol allowed, often by 1 to 2 weeks at a time.
That said, these data give me confidence that many patients may ultimately achieve 12- or even 16-week intervals. The ability to extend treatment while maintaining visual and anatomic outcomes is encouraging.
Of course, treatment remains individualized. I evaluate each patient's vision and OCT findings and extend only when I am confident the disease is stable.
One of the remaining questions is how much further patients can be extended beyond 64 weeks. RVO likely represents the highest VEGF burden among the retinal vascular diseases we treat, making long-term disease control particularly challenging.
Dr. Singer: Any final thoughts?
Dr. Fein: The key takeaway is that the visual acuity and anatomic improvements achieved by week 36 were maintained through week 64 across all treatment arms.
However, patients treated with aflibercept 8 mg received up to 3.2 fewer injections than those treated with aflibercept 2 mg. More patients in the 8-mg groups were fluid-free at week 64, and approximately threefold fewer required every-4-week dosing.
About 80% of patients treated with aflibercept 8 mg achieved treatment intervals of at least 12 weeks, and 40.5% of patients in the 3-loading-dose group achieved a final assigned interval of 20 weeks.
Importantly, the safety profile of aflibercept 8 mg was consistent with the established safety profile of aflibercept 2 mg.
Dr. Singer: This is very encouraging information. As we continue to manage what is often one of our most challenging retinal vascular diseases, a therapy that offers greater durability without compromising efficacy could be an important addition to our treatment options. Thank you for sharing these data with us.
Dr. Fein: Thank you for the opportunity. RP

