







Hydroxychloroquine (HCQ), sold under the trade name Plaquenil (Sanofi), is an immunomodulating drug indicated for conditions such as systemic lupus erythematosus (SLE), rheumatoid arthritis, and several other autoimmune diseases.1,2 HCQ exerts immunosuppressive effects by disrupting lysosomal activity, autophagy, and cytokine modulation. Retinal toxicity associated with HCQ use is well documented in the literature, primarily affecting the retinal pigment epithelium (RPE) and photoreceptor layers. When administered at recommended dosages, the cumulative risk of HCQ toxicity is less than 1% at 5 years and remains below 2% at 10 years; however, the risk increases markedly to approximately 20% after 20 years of continuous exposure. Major risk factors for HCQ toxicity include higher medication doses, long duration of use, renal disease, and tamoxifen use.3
Although studies on genetic susceptibility to HCQ-induced retinal toxicity are limited, one recent study identified several potential susceptibility genes, including RP1L1, RPGR, RPE65, and CCDC6, associated with CQ/HCQ retinopathy.4 Lecithin retinol acyltransferase (LRAT) is a key enzyme in the visual cycle that catalyzes the production of retinyl esters, which are essential for generating the visual chromophore required for phototransduction.5 Disruption of any component of the visual cycle, through drug toxicity, enzyme inactivation, or vitamin deficiency, can cause visual disturbances. This report presents a case of HCQ-associated retinal toxicity potentially amplified by a heterozygous LRAT gene mutation, highlighting the interplay between pharmacologic exposure and genetic predisposition.
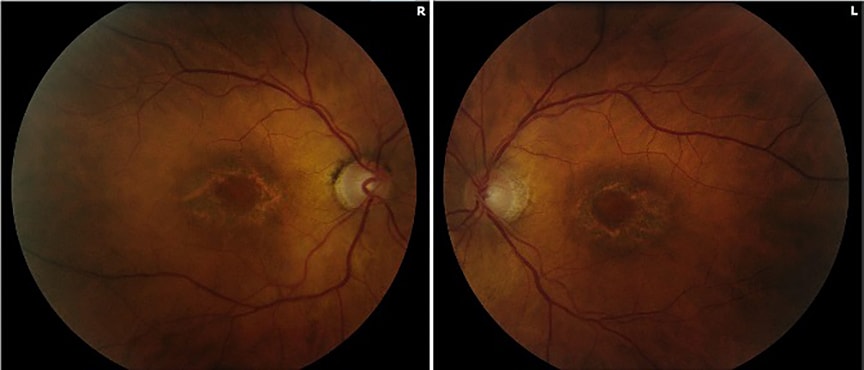
Figure 1. Fundus color imaging at initial presentation demonstrating bilateral bull’s-eye retinal pigment epithelium changes consistent with hydroxychloroquine retinopathy.
Case Presentation
A 70-year-old White female with a medical history notable for CREST syndrome, pulmonary hypertension, and lung transplant presented with severe blurry vision and intermittent flashes of light in both eyes. Family history was notable for neovascular age-related macular degeneration (nAMD) in her mother and brother. The patient had taken HCQ for 5 to 6 years and discontinued the medication after a physician at an outside clinic noted likely HCQ retinopathy. She had not taken HCQ for 4 years prior to the presentation described here.
On initial examination, best-corrected visual acuity (BCVA) was 20/70-2 in the right eye and 20/30-2 in the left eye. Slit lamp examination revealed no abnormalities in the anterior chamber. Posterior segment examination was notable for bilateral bull’s-eye retinal pigment epithelium (RPE) changes. Fundus imaging redemonstrated bull’s-eye RPE changes (Figure 1), and fluorescein angiography showed transmission defects consistent with these findings (Figure 2). Fundus autofluorescence demonstrated decreased autofluorescence bilaterally. These findings were consistent with HCQ retinopathy in both eyes.
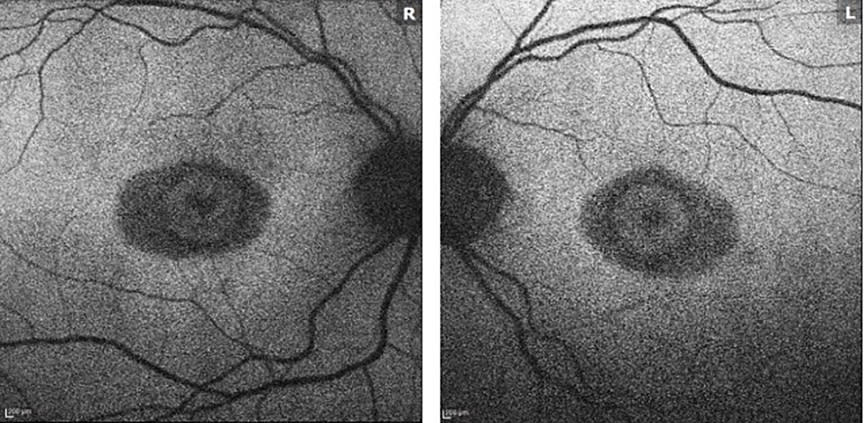
Figure 2. Fundus autofluorescence imaging demonstrating decreased autofluorescence bilaterally, consistent with hydroxychloroquine retinopathy.
The clinical team initiated dorzolamide ophthalmic solution 2% 3 times daily in the right eye for macular edema. Over the following 2 years, BCVA remained stable at 20/60 in the right eye and 20/40 in the left eye with correction. Three years after the initial presentation, her vision deteriorated to 20/150-1/+2 in the right eye, improving to 20/100-1/+1 with pinhole testing, and 20/100+1 in the left eye with no improvement on pinhole examination. Repeat OCT macula imaging showed ellipsoid zone disruption.
Because the patient had discontinued HCQ 7 years earlier, progression of retinopathy raised concern for an underlying genetic macular dystrophy. Genetic testing revealed a heterozygous LRAT gene mutation.
Discussion
The visual cycle is a biochemical pathway responsible for the continuous regeneration of 11-cis-retinal, the chromophore required for light detection in photoreceptor cells. Vitamin A plays a pivotal role in this process as the precursor for retinal chromophores. Additionally, LRAT and organic anion transporting polypeptide 1A2 (OATP1A2) are critical regulators of vitamin A metabolism and transport within the retina.6 Deficiencies in these components can disrupt retinoid recycling, leading to retinal dystrophies and impaired vision (Figure 3).
Vitamin A (all-trans-retinol [atROL]) undergoes enzymatic transformation after entering RPE cells via the STRA6 receptor, which binds retinol-binding protein (RBP) to mediate uptake from the bloodstream. LRAT then converts all-trans-retinol to retinyl esters. After transport to photoreceptor cells, these compounds contribute to the formation of rhodopsin in rods and photopsin in cones. Photon absorption triggers the phototransduction cascade, enabling visual perception.7 Vitamin A deficiency can impair phototransduction and cause nyctalopia. LRAT regulates the intracellular reservoir of retinoids, allowing regeneration of visual chromophores. The patient’s heterozygous LRAT mutation may have impaired her ability to generate the storage form of vitamin A, contributing to depletion of retinoid stores and worsening visual acuity.
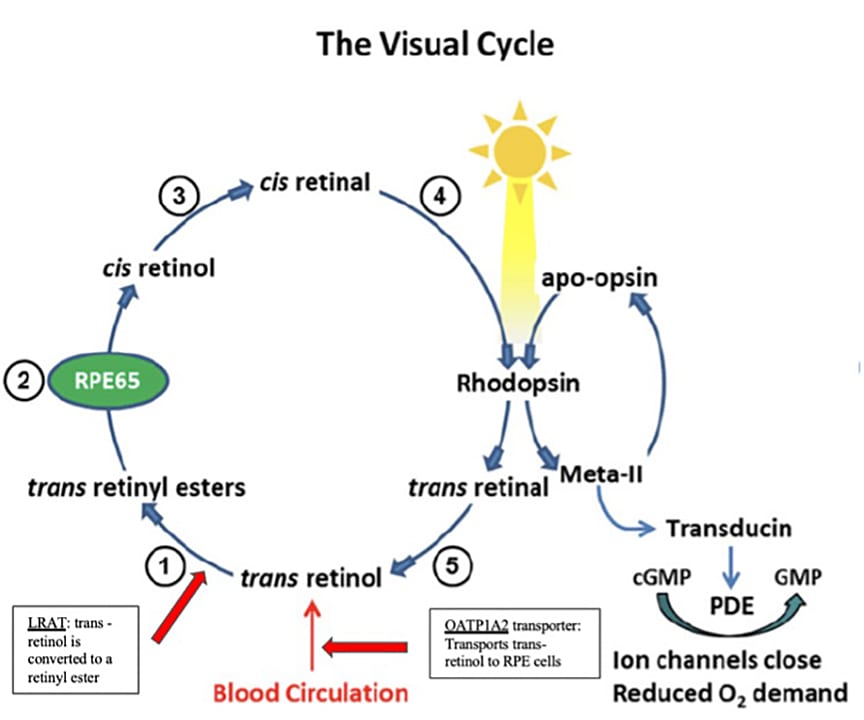
Figure 3. Schematic of the visual cycle depicting the isomerization of cis-retinal to trans-retinal, activation of rhodopsin, and initiation of the phototransduction cascade. Red arrows indicate points within the visual cycle involving the LRAT gene and the OATP1A2 transporter. Reproduced under Creative Commons Attribution (CC BY) license from Bavik C, Henry SH, Zhang Y, et al. Visual cycle modulation as an approach toward preservation of retinal integrity. PloS One. 2015;10(5):e0124940. doi:10.1371/journal.pone.0124940
OATP1A2 is a membrane transporter expressed on the apical membrane of RPE cells that facilitates uptake of atROL. It transports retinoids directly from the extracellular space into cells. HCQ has been shown to inhibit OATP1A2, resulting in extracellular accumulation of atROL, reduced availability for 11-cis-retinal regeneration, and disruption of the visual cycle.8 Notably, this protein is also involved in transport of drugs such as methotrexate and imatinib, indicating the potential for dangerous interactions with HCQ or reduced therapeutic potency due to inadequate transport to the target site. When HCQ is prescribed for autoimmune disease, thorough medication reconciliation is essential to identify drug-drug interactions that could exacerbate retinal pathology.
HCQ’s strong affinity for melanin leads to prolonged accumulation within the RPE, impaired cellular clearance, photoreceptor degeneration, and choroidal thinning. This manifests clinically as the characteristic bull’s-eye maculopathy, which may persist even after discontinuation of the drug.3,9 HCQ’s affinity for melanin may have contributed to this patient’s retinal toxicity because she had discontinued HCQ use 4 years prior to presentation. Progressive severe retinopathy has been documented for up to 20 years after cessation of HCQ therapy, suggesting that a metabolic insult may chronically destabilize cellular function rather than cause damage solely attributable to retained HCQ concentrations.10 Although the LRAT mutation alone does not fully explain the patient’s phenotype, HCQ exposure and the LRAT mutation may have acted synergistically to accentuate retinal toxicity beyond what would be expected from remote HCQ exposure alone. Although LRAT mutations and HCQ exposure individually have been associated with RPE damage, their combined effects have not previously been documented.
Conclusion
This case highlights the importance of intensified ophthalmologic monitoring in patients with genetic predispositions and raises the question of whether genetic screening should be considered before initiating medications associated with retinal toxicity. Although the American Academy of Ophthalmology recommends a baseline fundus examination and annual screening beginning after 5 years of HCQ use, clinicians may consider earlier and more frequent screening in patients with genetic risk factors.3 Genetic testing should also be considered in cases of atypical HCQ-associated or other drug-induced retinal toxicity to identify underlying mechanisms that may exacerbate disease and guide timely intervention. Such screening may inform clinical management and prompt consideration of alternative pharmacologic therapies when appropriate. Further research should aim to identify genetic mutations associated with increased disease severity and explore potential gene targets for therapy. RP



References
1. Dima A, Jurcut C, Arnaud L. Hydroxychloroquine in systemic and autoimmune diseases: Where are we now? Joint Bone Spine. 2021;88(3):105143. doi:10.1016/j.jbspin.2021.105143
2. Hu C, Lu L, Wan JP, Wen C. The pharmacological mechanisms and therapeutic activities of hydroxychloroquine in rheumatic and related diseases. Curr Med Chem. 2017;24(20):2241-2249. doi:10.2174/0929867324666170316115938
3. Marmor MF, Kellner U, Lai TYY, Melles RB, Mieler WF, American Academy of Ophthalmology. Recommendations on screening for chloroquine and hydroxychloroquine retinopathy (2016 revision). Ophthalmology. 2016;123(6):1386-1394. doi:10.1016/j.ophtha.2016.01.058
4. Chiu HI, Cheng HC, Wu CC, et al. Exome sequencing and genome-wide association analyses unveils the genetic predisposition in hydroxychloroquine retinopathy. Eye (Lond). 2024;38(10):1926-1932. doi:10.1038/s41433-024-03044-x
5. Sears AE, Palczewski K. Lecithin retinol acyltransferase: a key enzyme involved in the retinoid (visual) cycle. Biochemistry. 2016;55(22):3082-3091. Doi:10.1021/acs.biochem.6b00319
6. Bavik C, Henry SH, Zhang Y, et al. Visual cycle modulation as an approach toward preservation of retinal integrity. PloS One. 2015;10(5):e0124940. Doi:10.1371/journal.pone.0124940
7. Chen Y, Clarke OB, Kim J, et al. Structure of the STRA6 receptor for retinol uptake. Science. 2016;353(6302):aad8266. Doi:10.1126/science.aad8266
8. Xu C, Zhu L, Chan T, et al. Chloroquine and hydroxychloroquine are novel inhibitors of human organic anion transporting polypeptide 1A2. J Pharm Sci. 2016;105(2):884-890. Doi:10.1002/jps.24663
9. Ahn SJ, Ryu SJ, Joung JY, Lee BR. Choroidal thinning associated with hydroxychloroquine retinopathy. Am J Ophthalmol. 2017;183:56-64. Doi:10.1016/j.ajo.2017.08.022
10. Pham BH, Marmor MF. Sequential changes in hydroxychloroquine retinopathy up to 20 years after stopping the drug: implications for mild versus severe toxicity. Retina. 2019;39(3):492-501. Doi:10.1097/IAE.0000000000002408