







Polypoidal choroidal vasculopathy (PCV) is a distinct choroidal vascular disorder initially described in middle-aged Black women who presented with recurrent subretinal and subretinal pigment epithelium (RPE) hemorrhages.1 Although historically reported predominantly in Afro-Caribbean and Asian populations, recent studies have documented PCV in White patients, broadening recognition of the disease globally.2 Established risk factors include smoking, male sex, higher body mass index, hyperlipidemia, hypertension, and elevated serum inflammatory markers, such as C-reactive protein.3 Genetic studies suggest that PCV-associated loci involve the complement cascade, inflammatory pathways, extracellular matrix and basement membrane regulation, and lipid metabolism.4
Previous terminology for PCV includes idiopathic polypoidal vasculopathy, numerous recurrent serosanguinous RPE detachments, posterior uveal hemorrhage syndrome,5 and peripheral exudative hemorrhagic chorioretinopathy.6 Despite this varied nomenclature, these entities represent overlapping phenotypes of a single disease spectrum, providing historical context for current understanding.
Since its initial description, the clinical nature and pathogenesis of PCV have remained subjects of debate. Early reports suggested that the vascular lesions were situated in the inner choroid beneath Bruch’s membrane, based on angiographic findings and clinical observations.7 More recently, PCV is often considered a variant of age-related macular degeneration (AMD), although features such as drusen, pigmentary changes, and geographic atrophy are uncommon. Histologic and imaging studies support the theory that PCV represents a form of type 1 neovascularization rather than a primary choroidopathy, with neovascular complexes situated between the RPE and Bruch’s membrane.8

Figure 1. Multimodal imaging in a 64-year-old male with polypoidal choroidal vasculopathy. Fundus photography (A) shows subretinal hemorrhage involving the macula. Indocyanine green angiography (B) demonstrates 2 focal nodular areas of hypercyanescence, consistent with polypoidal lesions. Optical coherence tomography (C) reveals multiple pigment epithelial detachments with associated subretinal fluid and hemorrhage.
When to Suspect PCV in the Clinic
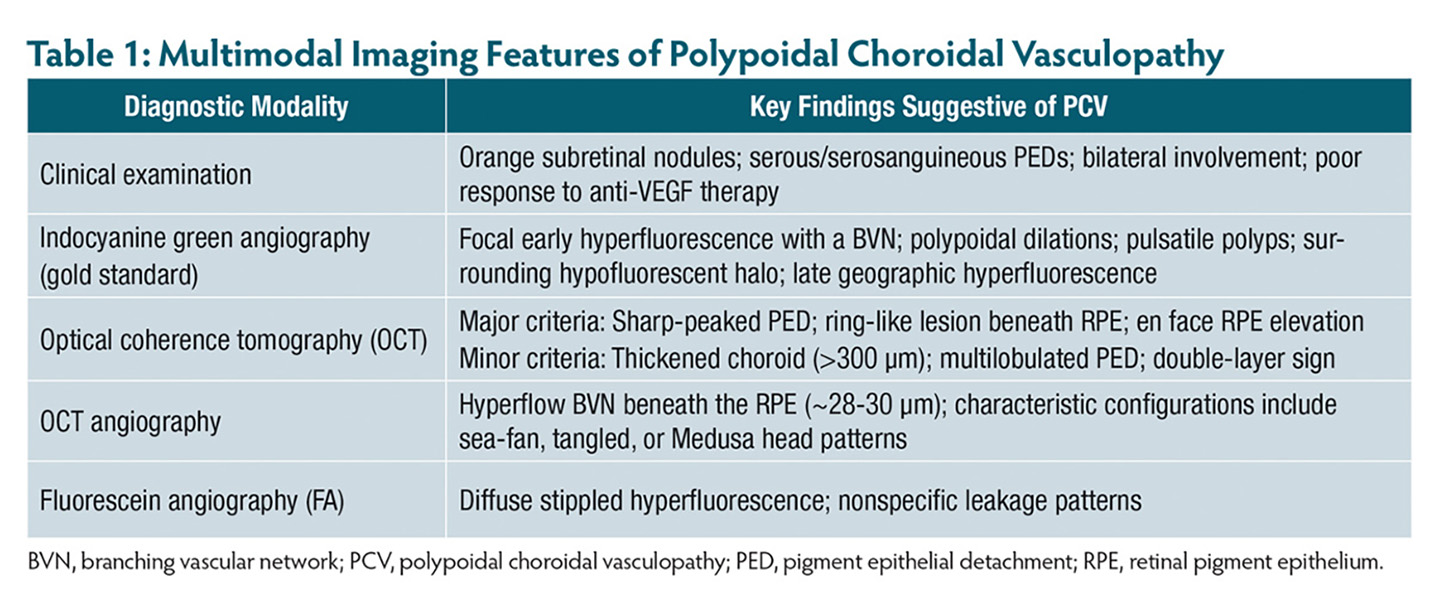
PCV should be considered in patients presenting with characteristic choroidal vascular lesions, particularly when conventional treatments yield suboptimal results. The dilated choroidal vascular channels that terminate in polyps appear clinically as orange, nodular lesions, most commonly located in the macula and peripapillary region. These lesions are frequently associated with serous or serosanguineous pigment epithelial detachments (PEDs).9 Micro-rips at the margins of PEDs10 and the presence of drusen in 23% to 55% of cases11 have also been observed. Despite these findings, presenting visual acuity is often relatively preserved due to minimal damage to intraretinal structures or extrafoveal lesion location. Bilateral involvement is common.12
Peripheral polyps may cause peripheral exudative hemorrhagic chorioretinopathy, most frequently in the temporal periphery. Although many peripheral polyps are benign and self-resolving, some can cause subretinal hemorrhage that threatens the macula and requires urgent intervention.13 A poor or incomplete response to anti-VEGF therapy is an important clinical clue that may help differentiate PCV from other chorioretinal disorders.14 Race, lesion location, response to therapy, and multimodal imaging can all contribute to an accurate diagnosis.

Figure 2. Multimodal imaging in a 65-year-old man with polypoidal choroidal vasculopathy. Fundus photography (A) shows a scar temporal to the optic nerve and along the inferior arcade, with surrounding suprachoroidal hemorrhage. Indocyanine green angiography (B) demonstrates focal hypercyanescence nasal to the optic disc, suggestive of a polyp. Optical coherence tomography (C) shows extensive pigment epithelial detachments, most prominent nasally.
Diagnostic Criteria
PCV diagnosis requires focal hyperfluorescence associated with at least 1 of the following: abnormal branching vascular network (BVN), nodular appearance on stereoscopic examination, orange retinal nodule, hypofluorescent halo, pulsatile polyp, or large submacular hemorrhage.15 Indocyanine green angiography (ICGA) is the gold standard for PCV diagnosis, identifying the BVN within the choroidal circulation and polypoidal dilations at vessel borders.16,17 Choroidal vascular hyperpermeability is more frequently observed in PCV than in other forms of choroidal neovascularization (CNV).18 Late geographic hyperfluorescence—a well-demarcated hyperfluorescent lesion that appears approximately 10 minutes after ICGA dye injection—is another characteristic finding.19 Nearly all eyes with PCV demonstrate late geographic hyperfluorescence, compared with only 7.5% of eyes with exudative AMD.20 Its presence in the fellow eye, even without a BVN, may indicate preclinical PCV.9
Advances in imaging techniques have led to a paradigm shift from ICGA-based diagnosis to a less invasive approach using optical coherence tomography (OCT). The Asia-Pacific Ocular Imaging Society validated non-ICGA diagnostic criteria, identifying 3 major OCT features with high specificity (91%) and positive predictive value (93%):
- ring-like lesions beneath the RPE;
- en face OCT complex RPE elevations corresponding to a BVN; and
- sharp-peaked PEDs.21
Additional minor criteria include thick choroid with dilated Haller vessels, complex or multilobular PED, and double-layer sign (separation of Bruch’s membrane and RPE by the BVN).22 Enhanced-depth imaging OCT often shows choroidal thickness >300 μm.23,24 This multimodal, noninvasive approach achieves an overall diagnostic accuracy of 82%, effectively distinguishing PCV from typical neovascular AMD when ICGA is unavailable (Figures 1 and 2).13
OCT angiography (OCTA) further improves BVN visualization, revealing hyperflow structures with a detection rate of 55% to 100%.25 BVN flow is typically 28.6 μm below the RPE reference plane.26 Morphologies described include sea-fan, tangled, and Medusa-head patterns.27 Fundus fluorescein angiography (FFA) and ICGA together aid in mapping lesions and determining the greatest linear dimension (GLD), because ICGA alone may not fully visualize PEDs or neurosensory detachments.28-30 Tan and colleagues proposed categorizing PCV based on FFA and ICGA traits: PCV with leaky BVN, PCV with interconnecting channels, and PCV with nonleaking BVN (Table 1).30
Treatment Approaches
Historically, standard laser photocoagulation was an effective option for extrafoveal polypoidal lesions, achieving lesion regression, reduced exudation, and long-term visual acuity improvement before the advent of current multimodal therapies.31 Today, treatment options include photodynamic therapy (PDT), intravitreal anti-VEGF therapy, a combination of PDT and anti-VEGF, and laser photocoagulation. PDT involves intravenous infusion of verteporfin (Visudyne; Bausch + Lomb), which is activated with a low-intensity laser to induce localized closure of abnormal choroidal blood vessels.
OCT has been used to plan adjunctive rescue PDT without requiring ICGA. Teo et al reported marking near-infrared reflectance images on a 6×6 mm OCT B-scan to cover all polypoidal lesions (PLs) and branching vascular networks (BVNs), achieving coverage of 100% of the PL area and 90% of the BVN area in a single circular location.32
The EVEREST clinical trial demonstrated that PDT, alone or combined with ranibizumab (Lucentis; Genentech), improved polyp closure rates.16 Ranibizumab monotherapy achieved 28.6% closure, compared with 71.4% for PDT alone and 77.8% for PDT plus ranibizumab.33 Anti-VEGF monotherapy and combination therapy were further assessed in EVEREST II and PLANET.34 EVEREST II compared ranibizumab with combination ranibizumab plus PDT at baseline, while PLANET evaluated aflibercept (Eylea; Regeneron) with rescue PDT available after 3 months. At a year, both trials showed significant visual acuity improvement with anti-VEGF monotherapy; polyp closure rates were 34.7% (EVEREST II) and 38.9% (PLANET). The mean number of injections was 7.3 in EVEREST II and 8.1 in PLANET. The evidence suggests that combination therapy resulted in improved vision and achieved a higher rate of complete polyp regression with fewer anti-VEGF injections than monotherapy.35
The LAPTOP study demonstrated that intravitreal ranibizumab provided superior visual acuity outcomes compared with PDT, with benefits maintained up to 5 years.36,37 On the other hand, the EPIC study evaluated intravitreal aflibercept in eyes previously treated with ranibizumab or bevacizumab (Avastin; Genentech), showing stabilization or improvement of vision in 91% of cases over 6 months, along with substantial resolution of subretinal fluid, hemorrhage, polyps, and PEDs in most cases.38
The phase 3 HAWK and HARRIER trials showed that brolucizumab (Beovu; Novartis) was noninferior to aflibercept for visual acuity gains at 48 weeks in patients with neovascular AMD, while allowing >50% of eyes to maintain a 12-week dosing interval.39,40 In PCV subgroups, brolucizumab demonstrated superior anatomic outcomes, including greater reductions in retinal thickness and fluid, suggesting a potential to reduce treatment burden.41
Triple therapy combining PDT, intravitreal anti-VEGF, and corticosteroids has been reported to improve visual outcomes compared to PDT monotherapy. It also allows longer retreatment-free intervals by targeting both vascular and inflammatory components of the disease.42
Recently, Arnold-Vangsted et al reported that faricimab (Vabysmo; Genentech) achieves a polyp regression rate of 48.7% (95% CI, 32.5-65.0%), comparable to rates reported with aflibercept monotherapy.43 In the Japanese subgroup of the phase 3 TENAYA trial, faricimab demonstrated similar visual and anatomical efficacy to aflibercept every 8 weeks at 1 year in treatment-naïve patients with nAMD, with comparable safety profiles. Mean best-corrected visual acuity (BCVA) gains and reductions in central subfield thickness were similar between groups. Notably, faricimab demonstrated greater durability, with approximately 66% of patients maintained on 16-week dosing intervals and nearly 90% on ≥12-week intervals at week 48. These findings, consistent with global TENAYA and LUCERNE results, support faricimab monotherapy as an effective and durable option for PCV.44
Conclusion
For patients with symptomatic PCV, anti-VEGF monotherapy or a combination of anti-VEGF therapy and PDT may serve as the initial treatment approach. Level I evidence from the EVEREST II and PLANET studies demonstrated that anti-VEGF therapy, alone or combined with PDT, can achieve substantial visual improvements after a year. Newer anti-VEGF agents have also shown meaningful efficacy in PCV and PED-associated disease, supporting their potential use as monotherapy.
However, because of the favorable response of the polypoidal complex to PDT, the reduced number of total injections, and the known phenomenon of PCV that is resistant to anti-VEGF treatment, adjunctive PDT may provide superior anatomical and visual outcomes in some cases. Additionally, when patient monitoring or retreatment adherence is a problem, combination therapy may represent the best option.45 RP


References
- Goldhardt R, Rosen BS. Polypoidal choroidal vasculopathy. Curr Ophthalmol Rep. 2019;7(1):66-72. doi:10.1007/s40135-019-00201-4
- Sen P, Manayath G, Shroff D, et al. Polypoidal choroidal vasculopathy: an update on diagnosis and treatment. Clin Ophthalmol Auckl NZ. 2023;17:53-70. doi:10.2147/OPTH.S385827
- Cho BJ, Heo JW, Kim TW, et al. Prevalence and risk factors of age-related macular degeneration in Korea: the Korea National Health and Nutrition Examination Survey 2010-2011. Invest Ophthalmol Vis Sci. 2014;55(2):1101-1108. doi:10.1167/iovs.13-13096
- Chen H, Liu K, Chen LJ, Hou P, Chen W, Pang CP. Genetic associations in polypoidal choroidal vasculopathy: a systematic review and meta-analysis. Mol Vis. 2012;18:816-829.
- Kleiner RC, Brucker AJ, Johnston RL. The posterior uveal bleeding syndrome. Retina. 1990;10(1):9-17.
- Yannuzzi LA, Sorenson J, Spaide RF, Lipson B. Idiopathic polypoidal choroidal vasculopathy (IPCV). Retina. 1990;10(1):1-8.
- Yannuzzi LA, Wong DW, Sforzolini BS, et al. Polypoidal choroidal vasculopathy and neovascularized age-related macular degeneration. Arch Ophthalmol. 1999;117(11):1503-1510. doi:10.1001/archopht.117.11.1503
- Kim JH, Kang SW, Kim TH, et al. Structure of polypoidal choroidal vasculopathy studied by colocalization between tomographic and angiographic lesions. Am J Ophthalmol. 2013;156(5):974-980.e2. doi:10.1016/j.ajo.2013.06.013
- Kumar A, Kumawat D, Sundar M D, et al. Polypoidal choroidal vasculopathy: a comprehensive clinical update. Ther Adv Ophthalmol. 2019;11:2515841419831152. doi:10.1177/2515841419831152
- Musashi K, Tsujikawa A, Hirami Y, et al. Microrips of the retinal pigment epithelium in polypoidal choroidal vasculopathy. Am J Ophthalmol. 2007;143(5):883-885. doi:10.1016/j.ajo.2006.12.024
- Ciardella AP, Donsoff IM, Huang SJ, et al. Polypoidal choroidal vasculopathy. Surv Ophthalmol. 2004;49(1):25-37. doi:10.1016/j.survophthal.2003.10.007
- Imamura Y, Engelbert M, Iida T, Freund KB, Yannuzzi LA. Polypoidal choroidal vasculopathy: a review. Surv Ophthalmol. 2010;55(6):501-515. doi:10.1016/j.survophthal.2010.03.004
- Goldman DR, Freund KB, McCannel CA, Sarraf D. Peripheral polypoidal choroidal vasculopathy as a cause of peripheral exudative hemorrhagic chorioretinopathy: a report of 10 eyes. Retina. 2013;33(1):48-55. doi:10.1097/IAE.0b013e31825df12a
- Fenner BJ, Cheung CMG, Sim SS, et al. Evolving treatment paradigms for PCV. Eye (Lond). 2022;36(2):257-265. doi:10.1038/s41433-021-01688-7
- Koh A, Lee WK, Chen LJ, et al. EVEREST study: efficacy and safety of verteporfin photodynamic therapy in combination with ranibizumab or alone versus ranibizumab monotherapy in patients with symptomatic macular polypoidal choroidal vasculopathy. Retina. 2012;32(8):1453-1464. doi:10.1097/IAE.0b013e31824f91e8
- Spaide RF, Yannuzzi LA, Slakter JS, et al. Indocyanine green videoangiography of idiopathic polypoidal choroidal vasculopathy. Retina. 1995;15(2):100-110. doi:10.1097/00006982-199515020-00003
- Yannuzzi LA, Ciardella A, Spaide RF, Rabb M, Freund KB, Orlock DA. The expanding clinical spectrum of idiopathic polypoidal choroidal vasculopathy. Arch Ophthalmol. 1997;115(4):478-485. doi:10.1001/archopht.1997.01100150480005
- Koizumi H, Yamagishi T, Yamazaki T, Kinoshita S. Relationship between clinical characteristics of polypoidal choroidal vasculopathy and choroidal vascular hyperpermeability. Am J Ophthalmol. 2013;155(2):305-313.e1. doi:10.1016/j.ajo.2012.07.018
- Kang SW, Chung SE, Shin WJ, Lee JH. Polypoidal choroidal vasculopathy and late geographic hyperfluorescence on indocyanine green angiography. Br J Ophthalmol. 2009;93(6):759-764. doi:10.1136/bjo.2008.145862
- Kim YT, Kang SW, Chung SE, et al. Development of polypoidal choroidal vasculopathy in unaffected fellow eyes. Br J Ophthalmol. 2012;96(9):1217-1221. doi:10.1136/bjophthalmol-2012-301644
- Laude A, Cackett PD, Vithana EN, et al. Polypoidal choroidal vasculopathy and neovascular age-related macular degeneration: same or different disease? Prog Retin Eye Res. 2010;29(1):19-29. doi:10.1016/j.preteyeres.2009.10.001
- Sato T, Kishi S, Watanabe G, et al. Tomographic features of branching vascular networks in polypoidal choroidal vasculopathy. Retina. 2007;27(5):589-594. doi:10.1097/01.iae.0000249386.63482.05
- Koizumi H, Yamagishi T, Yamazaki T, et al. Subfoveal choroidal thickness in typical age-related macular degeneration and polypoidal choroidal vasculopathy. Graefes Arch Clin Exp Ophthalmol. 2011;249(8):1123-1128. doi:10.1007/s00417-011-1620-1
- Hirami Y, Tsujikawa A, Otani A, et al. Hemorrhagic complications after photodynamic therapy for polypoidal choroidal vasculopathy. Retina. 2007;27(3):335-341. doi:10.1097/01.iae.0000233647.78726.46
- Tomiyasu T, Nozaki M, Yoshida M, Ogura Y. Characteristics of polypoidal choroidal vasculopathy evaluated by optical coherence tomography angiography. Invest Ophthalmol Vis Sci. 2016;57(9):OCT324-330. doi:10.1167/iovs.15-18898
- Chi YT, Yang CH, Cheng CK. Optical coherence tomography angiography for assessment of the 3-dimensional structures of polypoidal choroidal vasculopathy. JAMA Ophthalmol. 2017;135(12):1310-1316. doi:10.1001/jamaophthalmol.2017.4360
- Wang M, Zhou Y, Gao SS, et al. Evaluating polypoidal choroidal vasculopathy with optical coherence tomography angiography. Invest Ophthalmol Vis Sci. 2016;57(9):OCT526-532. doi:10.1167/iovs.15-18955
- Squirrell DM, Bacon JF, Brand CS. To investigate the prevalence of polypoidal choroidal vasculopathy in presumed age-related peripapillary subretinal neovascular membranes. Clin Experiment Ophthalmol. 2009;37(4):368-372. doi:10.1111/j.1442-9071.2009.02044.x
- Gomi F, Sawa M, Mitarai K, Tsujikawa M, Tano Y. Angiographic lesion of polypoidal choroidal vasculopathy on indocyanine green and fluorescein angiography. Graefes Arch Clin Exp Ophthalmol. 2007;245(10):1421-1427. doi:10.1007/s00417-007-0564-y
- Tan CSH, Ngo WK, Lim LW, Lim TH. A novel classification of the vascular patterns of polypoidal choroidal vasculopathy and its relation to clinical outcomes. Br J Ophthalmol. 2014;98(11):1528-1533. doi:10.1136/bjophthalmol-2014-305059
- Lee MW, Yeo I, Wong D, Ang CL. Argon laser photocoagulation for the treatment of polypoidal choroidal vasculopathy. Eye (Lond). 2009;23(1):145-148. doi:10.1038/sj.eye.6702955
- Chong Teo KY, Sadda SR, Gemmy Cheung CM, et al. Non-ICGA treatment criteria for suboptimal anti-VEGF response for polypoidal choroidal vasculopathy: APOIS PCV Workgroup Report 2. Ophthalmol Retina. 2021;5(10):945-953. doi:10.1016/j.oret.2021.04.002
- Koh A, Lai TYY, Takahashi K, et al. Efficacy and safety of ranibizumab with or without verteporfin photodynamic therapy for polypoidal choroidal vasculopathy: a randomized clinical trial. JAMA Ophthalmol. 2017;135(11):1206-1213. doi:10.1001/jamaophthalmol.2017.4030
- Lee WK, Iida T, Ogura Y, et al. Efficacy and safety of intravitreal aflibercept for polypoidal choroidal vasculopathy in the PLANET study: a randomized clinical trial. JAMA Ophthalmol. 2018;136(7):786-793. doi:10.1001/jamaophthalmol.2018.1804
- Takahashi K, Ohji M, Terasaki H, et al. Efficacy and safety of ranibizumab monotherapy versus ranibizumab in combination with verteporfin photodynamic therapy in patients with polypoidal choroidal vasculopathy: 12-month outcomes in the Japanese cohort of EVEREST II study. Clin Ophthalmol. 2018;12:1789-1799. doi:10.2147/OPTH.S171015
- Oishi A, Kojima H, Mandai M, et al. Comparison of the effect of ranibizumab and verteporfin for polypoidal choroidal vasculopathy: 12-month LAPTOP study results. Am J Ophthalmol. 2013;156(4):644-651. doi:10.1016/j.ajo.2013.05.024
- Miyamoto N, Mandai M, Oishi A, et al. Long-term results of photodynamic therapy or ranibizumab for polypoidal choroidal vasculopathy in LAPTOP study. Br J Ophthalmol. 2019;103(6):844-848. doi:10.1136/bjophthalmol-2018-312419
- Kokame GT, Lai JC, Wee R, et al. Prospective clinical trial of intravitreal aflibercept treatment for polypoidal choroidal vasculopathy with hemorrhage or exudation (EPIC study): 6-month results. BMC Ophthalmol. 2016;16:127. doi:10.1186/s12886-016-0305-2
- Dugel PU, Koh A, Ogura Y, et al. HAWK and HARRIER: phase 3, multicenter, randomized, double-masked trials of brolucizumab for neovascular age-related macular degeneration. Ophthalmology. 2020;127(1):72-84. doi:10.1016/j.ophtha.2019.04.017
- Cho HJ, Kang KH, Yoon W, Lee J, et al. Intravitreal brolucizumab and aflibercept for polypoidal choroidal vasculopathy. J Ocul Pharmacol Ther. 2023;39(9):653-660. doi:10.1089/jop.2023.0030
- Mori R, Honda S, Gomi F, et al. Efficacy, durability, and safety of faricimab up to every 16 weeks in patients with neovascular age-related macular degeneration: 1-year results from the Japan subgroup of the phase 3 TENAYA trial. Jpn J Ophthalmol. 2023;67(3):301-310. doi:10.1007/s10384-023-00985-w
- Ho M, Woo DCF, Chan VCK, et al. Treatment of polypoidal choroidal vasculopathy by photodynamic therapy, aflibercept and dexamethasone triple therapy. Sci Rep. 2016;6:36870. doi:10.1038/srep36870
- Arnold-Vangsted A, Schou MG, Balaratnasingam C, et al. Efficacy of intravitreal faricimab therapy for polypoidal choroidal vasculopathy: a systematic review and meta-analysis. Acta Ophthalmol. 2025;103(3):247-256. doi:10.1111/aos.16797
- Lai TYY, Lam CPS, Luk FOJ, et al. Photodynamic therapy with or without intravitreal triamcinolone acetonide for symptomatic polypoidal choroidal vasculopathy. J Ocul Pharmacol Ther. 2010;26(1):91-96. doi:10.1089/jop.2009.0073
- 45. Goldhardt R, Rosen BS. Polypoidal choroidal vasculopathy. Curr Ophthalmol Rep. 2019;7(1):66-72. doi:10.1007/s40135-019-00201-4