







Approaching retinal detachments (RDs) in patients with uveitis presents a unique set of challenges and requires careful perioperative and intraoperative planning. Patients with uveitis often present with complex detachments, and these occur more frequently in uveitic patients compared to those without uveitis.1 Additionally, these detachments are associated with higher rates of proliferative vitreoretinopathy (PVR) on presentation, lower success rates, worse final visual acuity, and higher rates of postoperative PVR development.1 Setting appropriate expectations for these patients is paramount before proceeding with surgery.
Inflammatory Control
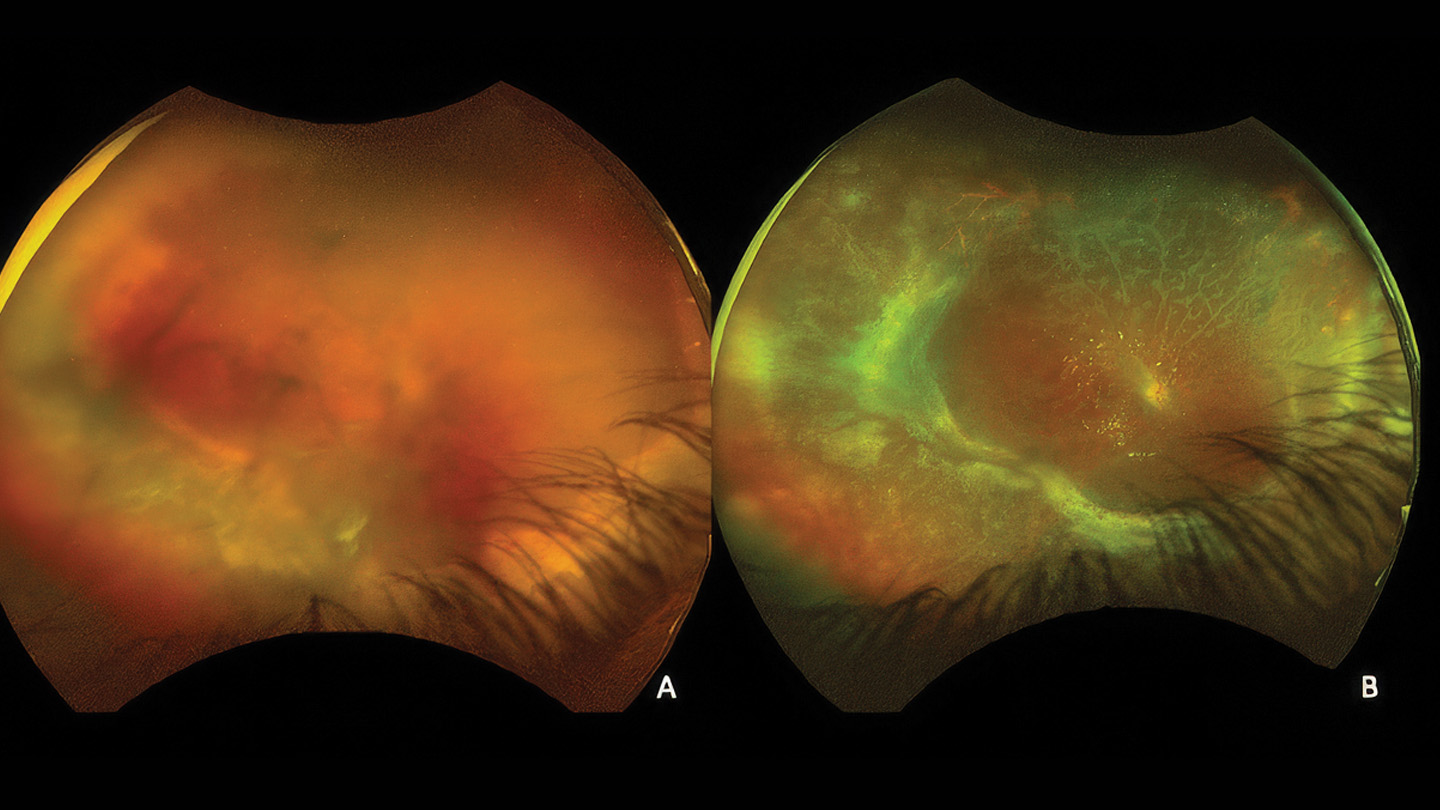
Figure 1. Acute retinal necrosis presenting in a patient with a moderate cataract and dense vitreous debris (A). Visualization was difficult due to a combination of cataract, vitreous cell, retinal whitening inferior. Surgical repair (B) involved scleral buckle, peripheral hyaloidal shave, inferior retinectomy, and silicone oil.
Traditionally, nonurgent surgery in uveitic eyes is deferred until the eye reaches quiescence, often with the aid of steroids or steroid-sparing immunotherapy. In ideal situations, quiescence is defined as a quiet anterior chamber and vitreous cavity. This definition also requires the absence of macular edema. The stringency of this definition stems from the potential sequelae that can develop when operating on an eye with active inflammation, including recalcitrant macular edema. Unfortunately, this level of inflammatory control is often not attainable in cases of RD, with reports documenting active inflammation in 46% of patients with uveitis undergoing RD surgery.1
In these situations, minimizing inflammation before surgery is essential to prevent as many lasting complications as possible. In cases of anterior noninfectious uveitis or scleritis, aggressive treatment with intravenous or oral corticosteroids for several days can provide coverage. This is because in these cases, post-operative inflammation can be quite impressive, and lead to cyclitic membrane formation, hypotony, and other complications.
If the disease is mostly posterior and noninfectious, management can be less intensive. In these circumstances, the main postoperative complication is macular edema, and local steroids after surgery can help achieve control.
Preoperative Exam and Imaging
Characterization of the detachment can also be difficult preoperatively. Particularly in eyes with intermediate or posterior uveitis, peripheral vitreoretinal traction can produce tiny retinal breaks that can be difficult to identify. This can create uncertainty regarding whether the detachment is exudative or rhegmatogenous. Widefield fundus photography can sometimes highlight peripheral pathology when a careful peripheral examination cannot. Enhanced-depth imaging optical coherence tomography can also demonstrate choroidal thickening beneath the detachment, which may suggest an inflammatory exudative process.
Clues such as shifting subretinal fluid, separate loculations of fluid, or improvement with steroid therapy may point toward an exudative process. It is important to note that in chronic RDs, subretinal fluid can become quite thick. This may cause a shifting appearance, complicating the preoperative assessment.
Another key point is that exudative detachments rarely occur in the setting of well-controlled intraocular inflammation. Therefore, in a patient with previously controlled uveitis who presents with a new detachment, even without an identifiable retinal break, a rhegmatogenous retinal detachment (RRD) is more likely. Occasionally, chronic RRDs can masquerade as exudative detachments with overlying inflammation. In these situations, inflammation may improve with corticosteroid therapy, but the subretinal fluid will not.2
Preoperative imaging, including ultrasonography and ultrasound biomicroscopy (UBM), can help assess areas of choroidal thickening, subretinal fluid, and fibrovascular membranes that may complicate cannula or infusion placement. Incorrect placement can result in iatrogenic retinal breaks and propagation of a retinal and/or choroidal detachment. In these situations, a 6-mm trocar may facilitate access to the vitreous cavity. In certain cases, rearranging the placement of cannulas may allow for successful infusion placement.
Intraoperative Considerations
Visualization is often challenging in these cases. A common cause is cataract progression, which can be accelerated by both steroids and inflammation. In cases of chronic detachment, staging cataract surgery before RD repair can be helpful. When this is not feasible, lensectomy may be performed at the time of RD surgery. Both approaches improve visualization and facilitate access to the vitreous base.
In cases requiring lens removal, it is reasonable to defer secondary intraocular lens implantation until after retinal reattachment. There is also an argument for complete capsular removal in these cases, because residual capsule can contribute to cyclitic membrane formation in the postoperative period.
Tamponade selection depends on several factors, including the status of the contralateral eye. Because uveitis is often a bilateral process, vision may already be limited in the nonsurgical eye. In such cases, a short-acting gas (if confident that all breaks are managed and can seal) or silicone oil may be an appropriate choice to preserve functional independence. Silicone oil can be particularly useful in eyes with inferior inflammatory membranes, residual traction, or multiple retinal breaks, such as those associated with infectious retinitis (Figure 1). However, silicone oil may interfere with the release of intravitreal injections, degrade visualization when intravitreal triamcinolone is used, and potentially serve as a scaffold for inflammatory membrane formation.
Retinal Detachment–Specific Considerations
In patients with RRD, tractional retinal detachment, or a mix of both, management is often similar to that in patients without uveitis. For eyes with multiple retinal breaks or inferior pathology, scleral buckle placement is often the best choice, with or without pars plana vitrectomy. A scleral buckle can also help support the peripheral retina, because the vitreous in these patients is often filled with inflammatory material, or in cases where the hyaloid is difficult to separate from the peripheral retina. Scleral buckle placement can be complicated in patients with prior uveitis, particularly scleral inflammation, because the sclera may be thinner. This may necessitate modification of the surgical plan, use of segmental elements, or abandonment of the buckle altogether if the risk of scleral perforation is substantial.
In cases of acute retinal necrosis, there is debate on the best approach. Some surgeons advocate early vitrectomy to clear inflammatory debris and relieve vitreoretinal traction before RD develops, whereas others prefer to wait until a detachment occurs. Early vitrectomy may improve visualization and facilitate monitoring for disease recurrence. However, concerns remain regarding the potential creation of additional retinal breaks and pathology.3
Patients with exudative RDs also require careful planning.2 Exudative detachments may occur in the setting of posterior scleritis, Vogt-Koyanagi-Harada (VKH) disease, and other inflammatory conditions. These detachments often result from subretinal fluid accumulation overlying an inflamed choroid.2 As noted previously, steroid therapy can reduce inflammation and resolve subretinal fluid, which may explain why visual outcomes in patients with exudative detachments are often better than in other forms of RD associated with uveitis.3
Differentiating between RRD and exudative RD is important for several reasons, particularly when considering scleral buckle placement. In predominantly exudative disease, scleral buckle placement may compress the choroid and potentially worsen the exudative process. In eyes with persistent exudative subretinal fluid after steroids or immunosuppression, surgical options may include pars plana vitrectomy or scleral windows.
Postoperative Considerations
Postoperative inflammation can lead to numerous complications. It is associated with increased rates of PVR, recurrent RD, macular edema, poorer visual outcomes, and postoperative hypotony. Therefore, the same principles used to achieve inflammatory control preoperatively should be maintained after surgery.
Patients with noninfectious uveitis can often be managed with a posterior sub-Tenon triamcinolone injection at the end of surgery, in addition to oral corticosteroids. In patients with infectious RDs, appropriate anti-infective therapy is essential if corticosteroids are used. As always, careful counseling regarding expectations before, during, and after surgery is critical. RP

References
1. Kerkhoff FT, Lamberts QJ, van den Biesen PR, Rothova A. Rhegmatogenous retinal detachment and uveitis. Ophthalmology. Feb 2003;110(2):427-31. doi:10.1016/s0161-6420(02)01744-x
2. Joye AS, Bhisitkul RB, Pereira DDS, Gonzales JA. Rhegmatogenous retinal detachment masquerading as exudative panuveitis with intense anterior chamber inflammatory reaction. Am J Ophthalmol Case Rep. Jun 2020;18:100618. doi:10.1016/j.ajoc.2020.100618
3. Surgical Panel, Retina Subspeciality Day, American Academy of Ophthalmology.