






The storied evolution of operating microscopes for intraocular surgery includes more than a century of landmark developments.1 Early advancements include the integration of stereo visualization by Zeiss Corporation in the 1890s, the first use of a binocular microscope for ophthalmic surgery in the 1940s, and gradual refinement in the 2000s with myriad innovations in optics, depth, and ease of use. These developments culminated in the more recent introduction of 3-dimensional (3D) visualization.2
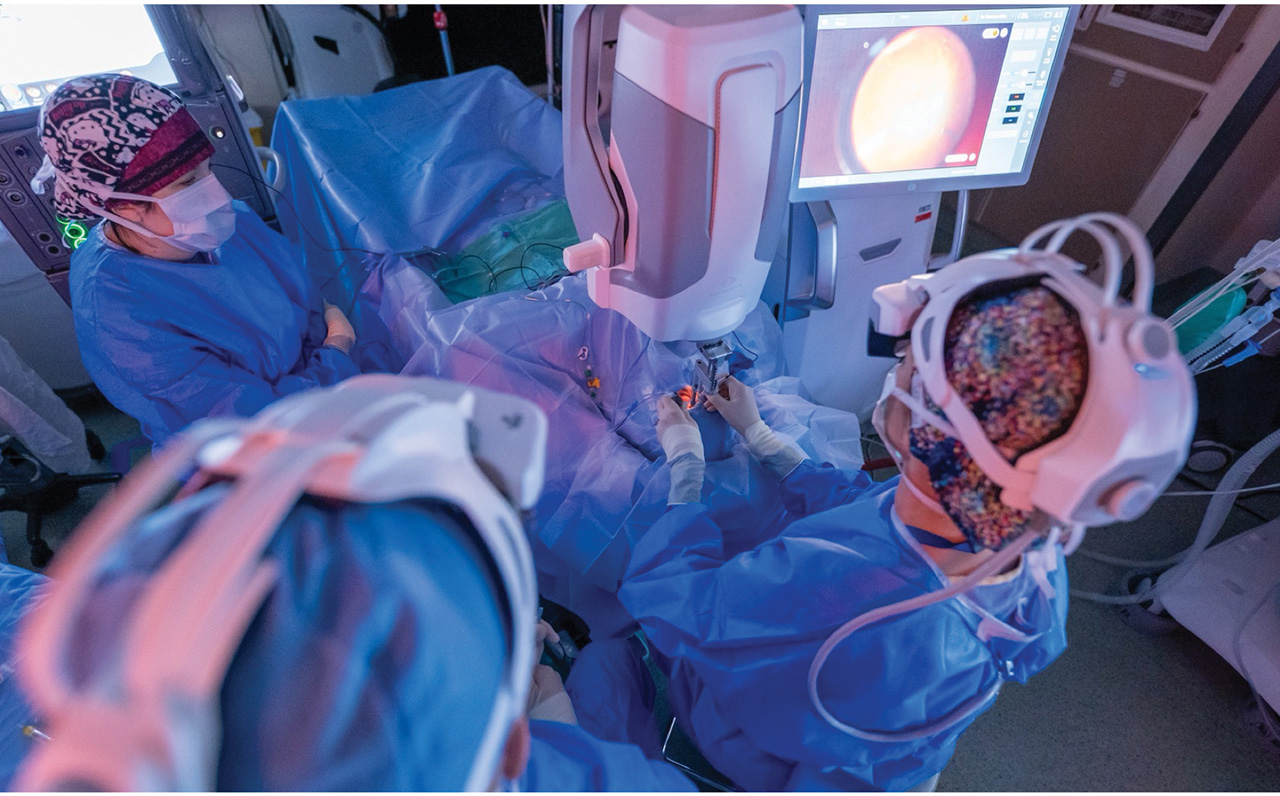
Figure 1A. Head-mounted display.
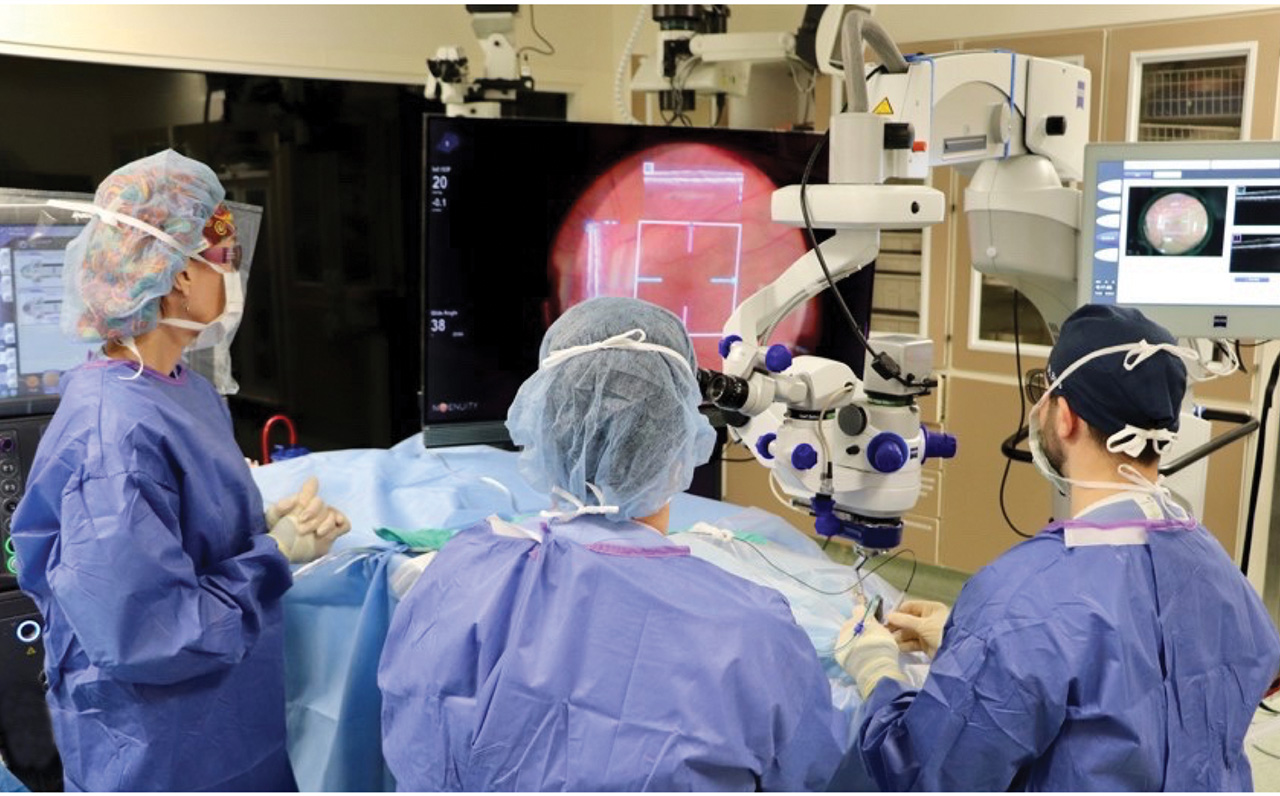
Figure 1B. Heads-up display.
3D systems have been developed to provide a digital stereoscopic view of the surgical field free from the constraints of microscope eyepieces using either a large high-definition display screen (Figure 1A) or head-mounted display (HMD) units (Figure 1B). 3D heads-up surgery offers benefits in ergonomics, efficiency, reduction in light exposure, and 3D visualization for all members of the surgical team. The systems carry risks of latency, surgical field limitations, color or image distortion, learning curve delay, peripheral viewing difficulty, and the cost and logistics of implementation. Interested surgeons should weigh these advantages and limitations before investing in a specific system.
Currently available systems include Artevo (Zeiss), Ngenuity (Alcon), SeeLuma (Bausch + Lomb), and Beyeonics One (Beyeonics Vision/BVI Medical). The safety and efficacy of these systems have been established, with multiple reports showing no clinical, anatomic, or visual acuity differences between 3D visualization systems and conventional microscopy in macular or retinal detachment surgeries.3-6 Ngenuity uses a 3D digital camera mounted on a standard scope, whereas Artevo is an integrated digital microscope. Both use flat panel display screens for heads-up viewing. Beyeonics One provides an augmented reality HMD which is fully digital and uses the exoscope, which is a hands-free scope with gesture controls. Beyeonics One features automatic focus, pan, and zoom. The HMD has case series evidence for safety and efficacy, with unique benefits from hands-free operation and associated nuances in learning curve.7,8 Although a head-to-head comparison of HMDs vs 3D monitors has not yet been performed, many of the benefits of 3D heads-up surgery are similar across devices, with most studies reporting on screen-based Ngenuity or Artevo systems.3

Figure 2. Heads-up display requiring perfect orientation of screens in operating room. Assistant surgeon must adopt a head turn to view operating screen.
Illumination
The lower illumination needed for digital systems may reduce theoretical risks of iatrogenic retinal light injury.9 Pars plana vitrectomy for retinal detachment repair with 3D systems can be completed under lower illumination intensity compared to traditional microscopes.10 Adjustments in optical parameter profiles may further facilitate visualization of epiretinal membrane or internal limiting membranes,11 potentially reducing the amount of intraoperative dye. 3D surgical systems purport higher depth of field compared to traditional microscopes, with some studies showing less intraoperative adjustments for membrane peeling in delicate macular surgeries.12
Ergonomics
Musculoskeletal disorders and back pain are well-known occupational risks to ophthalmologists.13,14 In terms of operating room ergonomics, standard microscopes are believed to promote head-forward and back-arched positioning that promotes muscle fatigue. This may be reduced in digital 3D systems.15 In addition to surveys showing improvement in back and neck pain, objective measures of neck and back muscle tone have shown improved ergonomics with digitally assisted systems.16 If these systems allow retinal surgeons to perform more surgeries, or continue their surgical careers without risk of chronic musculoskeletal issues, these systems may be well worth the investment.
Educational Value
3D surgical videos may have increased educational value compared to 2D recordings, especially for medical students and early learners.17 A survey of clinicians across the vitreoretinal surgical team found a generally positive impact of 3D displays during surgery, though there were worse reported user experiences when performing endolaser, closing, and scleral fixation of intraocular lenses.18 Further, pilot data suggest these systems could allow telesurgery,19 which could have significant implications for patient access, collaboration, and education.
Figure 3. Examples of viewing difficulty with current systems: endolaser difficulty with visualization of aiming beam (A), digitization artifact (B), difficulty with peripheral visualization (C), and oversaturated colors and misalignment with surgeon view (D).
Limitations
Early work with 3D heads-up display has also been shown to require longer macular peel times and less ease of use, which suggests a learning curve during adoption of the new technology.20 Similar reports show increased surgical duration with 3D systems for retinal detachment repair,21 which decreases with experience. Other studies have shown similar surgical timing with 3D systems.22 There may be surgeon-specific factors in utilization, and emerging trainees with more exposure to virtual or augmented reality outside of the operating room may find heads-up HMD more easily integrated into their practice. In any case, the potential for adjustment for all members of the surgical team should be considered.
There are additional notable shortcomings of 3D systems that should be considered by vitreoretinal surgeons. Headsets for surgeons and assistants could cause head discomfort or fogging from condensation and can introduce cumbersome additional steps in surgery if the headset or display is not used for the entire case (Figure 2). The machine must be properly positioned and could create obstacles in the operating room, including limiting anesthesia access to patients.18 Early reports of latency may be less clinically meaningful with improvements in engineering.23 Other considerations include possible distortion from digitized images or oversaturated colors, and challenges in peripheral viewing (Figure 3). Finally, 3D systems require variable capital expenditure, storage, maintenance, and integration of large new equipment into existing operating rooms. These investments may be administratively or logistically difficult, especially for cost-conscious ambulatory surgical settings, in lieu of robust improvements in clinical outcomes.

Figure 4. Integrated operating room with immersive digital visualization and iOCT (A) and head-mount display control (B).
Future Directions
Future innovations in 3D viewing systems may continue to augment the surgical experience. In the DISCOVER study, integration with 3D surgical visualization systems allowed simultaneous viewing of OCT and the surgical field (Figure 4).24 As a result, this system was shown to augment surgical visualization efficiency, with less illumination, and ergonomic benefits compared to conventional microscope intraoperative OCT.25,26 Similar findings are shown with HMDs, without the need for reverting to a conventional microscope.27 Future developments such as improved image processing software could fundamentally shift the risk-benefit calculus for adopting these systems. RP


References
1. Keeler R. The evolution of the ophthalmic surgical microscope. Hist Ophthal Intern. 2015;1:35-66.
2. Srinivasan S, Tripathi AB, Suryakumar R. Evolution of operating microscopes and development of 3D visualization systems for intraocular surgery. J Cataract Refract Surg. 2023;49(9):988-995. doi:10.1097/j.jcrs.0000000000001216
3. Ripa M, Kopsacheilis N, Kanellopoulou K, Nomikarios M, Motta L. Three-dimensional heads-up vs standard operating microscope for cataract surgery: a systematic review and meta-analysis. Diagnostics (Basel). 2022;12(9)doi:10.3390/diagnostics12092100
4. Kantor P, Matonti F, Varenne F, et al. Use of the heads-up NGENUITY 3D Visualization System for vitreoretinal surgery: a retrospective evaluation of outcomes in a French tertiary center. Sci Rep. 2021;11(1):10031. doi:10.1038/s41598-021-88993-z
5. Zhang T, Tang W, Xu G. Comparative analysis of three-dimensional heads-up vitrectomy and traditional microscopic vitrectomy for vitreoretinal diseases. Curr Eye Res. 2019;44(10):1080-1086. doi:10.1080/02713683.2019.1612443
6. Zeng R, Feng Y, Begaj T, Baldwin G, Miller JB. Comparison of the safety and efficacy of a 3-dimensional heads-up display vs a standard operating microscope in retinal detachment repair. J Vitreoretin Dis. 2023;7(2):97-102. doi:10.1177/24741264221150074
7. Iuliano L, Corbelli E, Bandello F, Codenotti M. Lessons from the vitreoretinal theater using the Beyeonics One surgical visualization system. Eur J Ophthalmol. 2025;35(6):1953-1957. doi:10.1177/11206721251349248
8. Schwartz S, Gomel N, Loewenstein A, Barak A. Use of a novel beyeonics one three-dimensional head-mounted digital visualization platform in vitreoretinal surgeries. Eur J Ophthalmol. 2024;34(3):880-883. doi:10.1177/11206721241229115
9. Adam MK, Thornton S, Regillo CD, Park C, Ho AC, Hsu J. Minimal endoillumination levels and display luminous emittance during three-dimensional heads-up vitreoretinal surgery. Retina. 2017;37(9):1746-1749. doi:10.1097/IAE.0000000000001420
10. Ge X, Liu D, Liu Y, et al. Comparing the randomized trial outcomes of 3d low-light intensity-assisted and traditional eyepiece-assisted pars plana vitrectomy for rhegmatogenous retinal detachment. Ophthalmic Res. 2025;68(1):90-99. doi:10.1159/000543135
11. Melo AGR, Conti TF, Hom GL, et al. Optimizing visualization of membranes in macular surgery with heads-up display. Ophthalmic Surg Lasers Imaging Retina. 2020;51(10):584-587. doi:10.3928/23258160-20201005-06
12. Zhang X, Hu H, Li W, et al. Objective quantification of depth-of-field advantage in 3D surgical video system for vitreoretinal surgery: safety and efficacy in macular diseases. Retina. 2024;44(5):878-886. doi:10.1097/IAE.0000000000004027
13. Dhimitri KC, McGwin G, Jr., McNeal SF, et al. Symptoms of musculoskeletal disorders in ophthalmologists. Am J Ophthalmol. 2005;139(1):179-81. doi:10.1016/j.ajo.2004.06.091
14. Chatterjee A, Ryan WG, Rosen ES. Back pain in ophthalmologists. Eye (Lond). 1994;8(Pt 4):473-474. doi:10.1038/eye.1994.112
15. Weinstock RJ, Ainslie-Garcia MH, Ferko NC, et al. Comparative assessment of ergonomic experience with heads-up display and conventional surgical microscope in the operating room. Clin Ophthalmol. 2021;15:347-356. doi:10.2147/OPTH.S292152
16. Park SJ, Hwang JM, Jae Jin Park E, Shin JP, Park DH. Comparison of surgeon muscular properties between standard operating microscope and digitally assisted vitreoretinal surgery systems. Retina. 2022;42(8):1583-1591. doi:10.1097/IAE.0000000000003482
17. Chhaya N, Helmy O, Piri N, Palacio A, Schaal S. Comparison of 2D and 3D video displays for teaching vitreoretinal surgery. Retina. 2018;38(8):1556-1561. doi:10.1097/IAE.0000000000001743
18. Shoshany TN, Agranat JS, Armstrong G, Miller JB. The user experience on a 3-dimensional heads-up display for vitreoretinal surgery across all members of the health care team: a survey of medical students, residents, fellows, attending surgeons, nurses, and anesthesiologists. J Vitreoretin Dis. 2020;4(6):459-466. doi:10.1177/2474126420929614
19. Lu ES, Reppucci VS, Houston SKS, 3rd, Kras AL, Miller JB. Three-dimensional telesurgery and remote proctoring over a 5G network. Digit J Ophthalmol. 2021;27(3):38-43. doi:10.5693/djo.01.2021.06.003
20. Talcott KE, Adam MK, Sioufi K, et al. Comparison of a three-dimensional heads-up display surgical platform with a standard operating microscope for macular surgery. Ophthalmol Retina. 2019;3(3):244-251. doi:10.1016/j.oret.2018.10.016
21. Asani B, Siedlecki J, Schworm B, et al. 3D heads-up display vs. standard operating microscope vitrectomy for rhegmatogenous retinal detachment. Front Med (Lausanne). 2020;7:615515. doi:10.3389/fmed.2020.615515
22. Giansanti F, Nicolosi C, Bacherini D, et al. Three-dimensional visualization system for vitreoretinal surgery: results from a monocentric experience and comparison with conventional surgery. Life (Basel). 2023;13(6). doi:10.3390/life13061289
23. Ta Kim D, Chow D. The effect of latency on surgical performance and usability in a three-dimensional heads-up display visualization system for vitreoretinal surgery. Graefes Arch Clin Exp Ophthalmol. 2022;260(2):471-476. doi:10.1007/s00417-021-05388-6
24. Ehlers JP, Uchida A, Srivastava SK. The integrative surgical theater: combining intraoperative optical coherence tomography and 3D digital visualization for vitreoretinal surgery in the DISCOVER study. Retina. 2018;38(Suppl 1):S88-S96. doi:10.1097/IAE.0000000000001999
25. Figueiredo N, Talcott KE, Srivastava SK, et al. Conventional microscope-integrated intraoperative OCT versus digitally enabled intraoperative OCT in vitreoretinal surgery in the DISCOVER study. Ophthalmic Surg Lasers Imaging Retina. 2020;51(4):S37-S43. doi:10.3928/23258160-20200401-05
26. Talcott KE, Knapp AN, Amine R, et al. Comparing three-dimensional digitally enabled intraoperative OCT with conventional microscope-integrated OCT in vitreoretinal surgery: a post hoc analysis of the DISCOVER study. Ophthalmic Surg Lasers Imaging Retina. 2024;55(5):270-277. doi:10.3928/23258160-20240206-01
27. Mizuno M, Matar K, Amine R, et al. The feasibility and clinical evaluation of an immersive augmented reality surgical headset integrated with swept-source intraoperative optical coherence tomography for ophthalmic surgery in the DISCOVER study. Diagnostics (Basel). 2025;15(11)doi:10.3390/diagnostics15111394