







Soon, it may be possible to inject an array of “microbots”—each smaller than 1/50th the width of a human hair—into the eye to treat retinal pathologies. Researchers at Applied Research Associates (ARA), a private scientific research and engineering firm, and Southern Methodist University (SMU) in Dallas are currently developing microbots to help mitigate damage from vitreous hemorrhages and shorten recovery times. This project, funded by grants from the US Department of Defense, aims to assist combat soldiers who are at a higher risk of vitreous hemorrhage than the general population. However, the technology is expected to have civilian applications as well. In our conversation, which has been edited for length and clarity, Louis William Rogowski, PhD, a senior research scientist at ARA, and Min Jun Kim, PhD, the Robert C. Womack Endowed Chair Professor at SMU’s Lyle School of Engineering, discussed how these microbots work and the challenges of this ambitious project.
Retinal Physician (RP): What is a microbot? How are nanotechnology and robotics evolving to enable precise, minimally invasive treatments like this?
Dr. Rogowski: A microbot is a biocompatible robotic system smaller than 1 mm in any dimension, designed to operate inside the human body and perform targeted, noninvasive interventions. The idea is to use swarms of these microbots to precisely deliver drug payloads to target sites inside the body such as tumors, blood clots, or other injuries. These have the potential to be more effective than conventional treatments, leveraging targeted drug delivery and minimally invasive surgical procedures to accomplish their tasks.
The field of microrobotics is presently undergoing a transition period, moving out of academic research into practical applications. Our current effort, [funded by] the Medical Technology Enterprise Consortium (MTEC) and the Science and Technology Enterprise Integration Division (STEID), Research and Engineering Directorate, Defense Health Agency, aims to bring microbots to the aid of the warfighter, allowing them to have accelerated recovery from vitreous hemorrhage injuries.
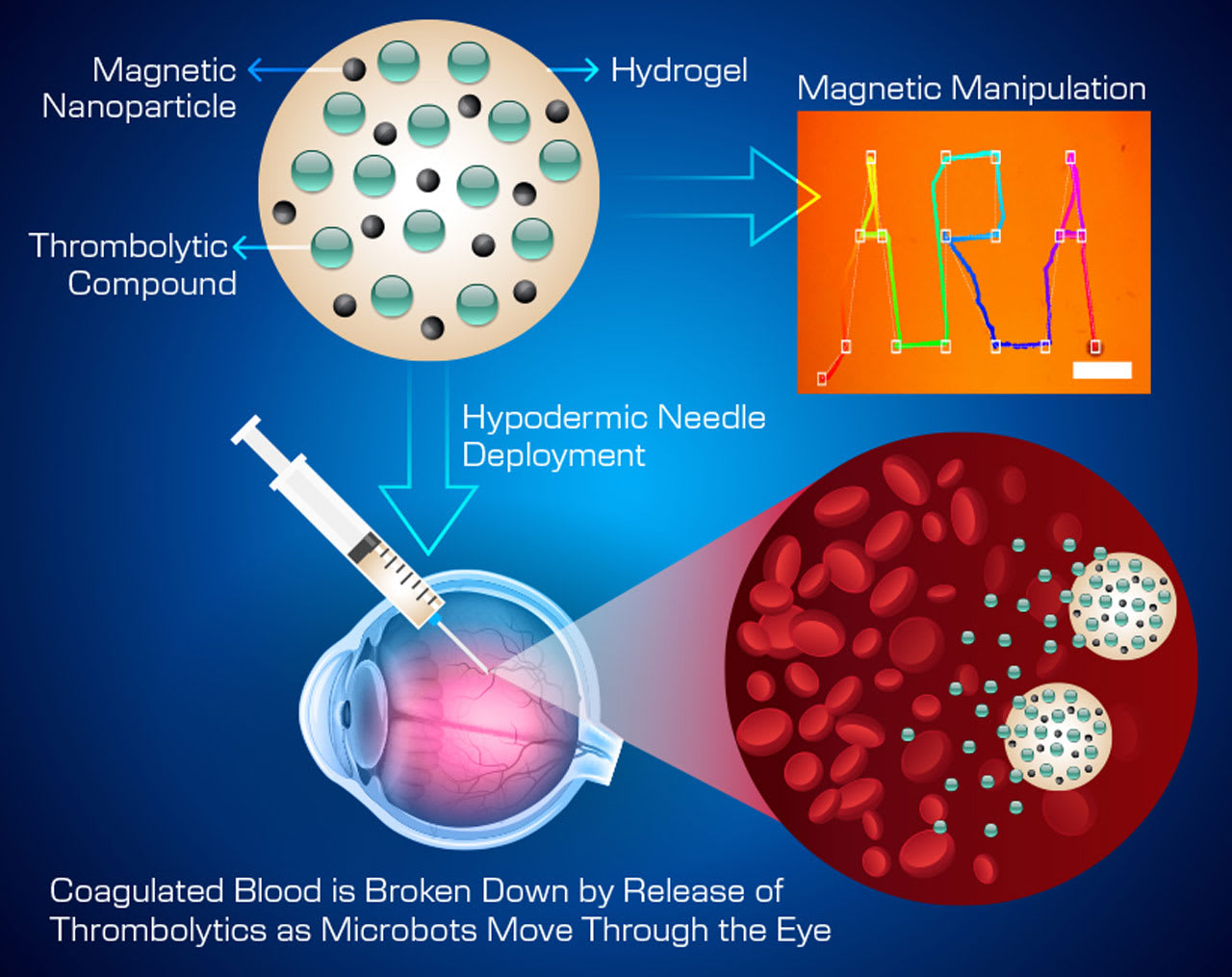
Figure 1. To treat vitreous hemorrhage, small-scale microrobots will be injected into the eye, where they will use targeted drug delivery to break down red blood cells.
RP: What will these microbots look like? How will they be delivered to the eye, and how will they work to break down red blood cells and accelerate recovery from vitreous hemorrhage?
Dr. Rogowski: The microbots being developed by ARA and SMU are soft, spherical hydrogel particles designed to encapsulate both magnetic components (biodegradable iron oxide nanoparticles) and therapeutic payloads. The robots themselves will be less than one tenth of a millimeter in diameter and be injected en masse into affected eyes using a hypodermic needle. The microbots will release thrombolytic compounds through squeezing out of the hydrogel, which will be tailored to allow for enhanced release rates under physiologic temperatures (98.6°F/37°C). Under magnetic navigation, the hydrogel swarms will be precisely navigated to red blood cell “floaters” inside the vitreous humor (Figure 1). These floaters would normally persist for months after a vitreous hemorrhage, but using our technique we are hoping to rapidly decrease recovery time for patients.
RP: What are the main engineering challenges when it comes to designing and controlling microrobots? Are any retina specialists providing input into their development?
Dr. Rogowski: One of the major challenges in medical microrobots is how can they be effectively visualized inside the body? For gastrointestinal cancers or blood-brain barrier interactions, the answer isn’t straightforward. Inside the eyes, however, where tools already exist for visualization, the challenge decreases. ARA and SMU have each developed magnetic control systems tailored for navigating microbots through biofluids. Now, both institutions are collaborating to advance precise 3D tracking and coordinated swarm control of these microbots using integrated visual and magnetic detection techniques.
In addition to ARA and SMU, we are using consultants from the University of Colorado Anschutz Medical Campus to support our effort. Dr. Christene Huang is a trained transplant immunologist with more than 25 years of experience in the field, and Dr. Natalia Vergara is an ophthalmologist with decades of experience researching retinal degenerative diseases. Of course, ensuring biocompatibility, uniform drug loading, and that no damage occurs to sensitive ocular structures remain challenges as well.
RP: How does this approach aim to overcome the limitations of current treatment methods for vitreous hemorrhage?
Dr. Kim: It is our intention to create a recovery technique that is significantly faster than typical recovery times for vitreous hemorrhages. Without assistance, floaters inside the eye will be naturally cleared from the eye at a rate of approximately 1% per day, which can lead to months of diminished vision or total vision loss after injury. Although treatments exist like vitrectomy, which removes the gel of the vitreous humor and replaces it with a saline solution, full vision restoration would still take upwards of a month. Vitrectomy can also in some cases create excessive ocular pressure, retinal detachment, and other serious side effects. Although the microbot use case is still very early in development, it is our hope that this technology will lead to safer and more effective treatment options for both civilian and military populations.
RP: What steps in development and testing do you anticipate before these microrobots could be considered for clinical use? Is there a timetable for this program?
Dr. Kim: Right now, we are still early in this process. It is our intention by the end of this program to demonstrate the totality of the treatment strategy within postmortem eyes from animal models. The project is broken down into 6-month sprints, with the first 6 months dedicated to nailing down the hydrogel formulation and release rates of thrombolytics from microbots. Next, we’ll explore swarm control and navigation of the microbots to precisely target and degrade blood clots within artificial ocular model chambers. Finally, we’ll introduce the microbots and therapeutic agents into postmortem animal eyes to validate and refine the previous research phases. Upon successful completion of these steps, we’ll progress to in vivo studies, with the goal of advancing toward clinical trials.
RP: What does success look like for this project, and what milestones do you hope to achieve by the end of this effort?
Dr. Rogowski: By the end of this effort, we’ll have developed a microbot formulation and fabrication strategy tailored for thrombolytic delivery, along with advanced control algorithms for targeting red blood cells and clots within ocular environments. Additionally, we’ll generate a comprehensive set of preclinical data to support the transition toward human trials. We also aim to publish high-quality technical journal papers and share our findings at leading conferences.
RP: Beyond vitreous hemorrhage, do you see potential applications for microbot technology in other areas of ophthalmology?
Dr. Kim: We are open to exploring new applications—both within ophthalmology and beyond, including potential use in health care and industry. For now, our primary focus is on successfully accomplishing our current goals. Once we have demonstrated strong performance in this area, expanding into other applications will be a much more seamless transition. RP
Editor’s note: This project is sponsored by the Medical Technology Enterprise Consortium (MTEC) and the Science and Technology Enterprise Integration Division (STEID), Research and Engineering Directorate, Defense Health Agency. This effort is fully sponsored by the Government under Other Transaction Number W81XWH-15-9-0001.
The views and conclusions contained herein are those of the authors and should not be interpreted as necessarily representing the official policies or endorsements, either expressed or implied, of the US government.