







VOY-101, a one-time intravitreal gene therapy designed to restore complement regulation in patients with geographic atrophy (GA), has advanced into phase 2 testing following a pair of early studies that suggest the treatment could achieve sustained intraocular expression with a well-tolerated safety profile.
At the 2026 Association for Research in Vision and Ophthalmology (ARVO) meeting in Denver, Charles C. Wykoff, MD, PhD, of Retina Consultants of Texas, presented data from the phase 1 studies for the AAV2-based gene therapy being developed by Perceive Biotherapeutics. He explained that the treatment is intended to augment complement regulation through expression of a form of truncated “protective” complement factor H protein found in patients who are less susceptible to AMD.

Figure 1. VOY-101 is designed for GA to deliver protective CFHT transgene that localizes to the RPE cell surface and promotes inactivation of excess C3b, with the goal of reducing MAC deposition and protecting RPE cells from complement-mediated damage. The slide illustrates the genetic rationale underlying the therapy, including enhanced CFH surface binding associated with protective CFH variants and reduced complement amplification at the level of the RPE.
The therapy is being initially studied among patients with GA with higher AMD genetic risk to control the dysregulation of the alternative complement pathway that leads to GA. According to Dr. Wykoff, the treatment strategy was informed not only by genetic studies explaining susceptibility to AMD, but also by research examining why some patients do not develop advanced disease. “That work led to the discovery of protective CFH haplotypes,” he said. “It’s that deep understanding of these genetics and subsequent function that led to the design of the VOY-101 gene therapy” (Figure 1).
VOY-101 was evaluated in 2 parallel multicenter open-label phase 1 studies, PBI-AMD-001 and PBI-AMD-002. The dose-escalation and extension studies enrolled patients aged 60 years or older with CFH genetic risk and GA lesion sizes ranging from 2.5 mm² to 20 mm². Patients received a single intravitreal injection across 6 dose levels, followed by a 24-week topical steroid taper (Figure 2). Across the 24 treated patients, mean age was 77.6 years and mean baseline GA lesion size in the study eye was 9.8 mm². Mean follow-up at the time of analysis was 633 days, with 17 patients completing 24 months of follow-up.
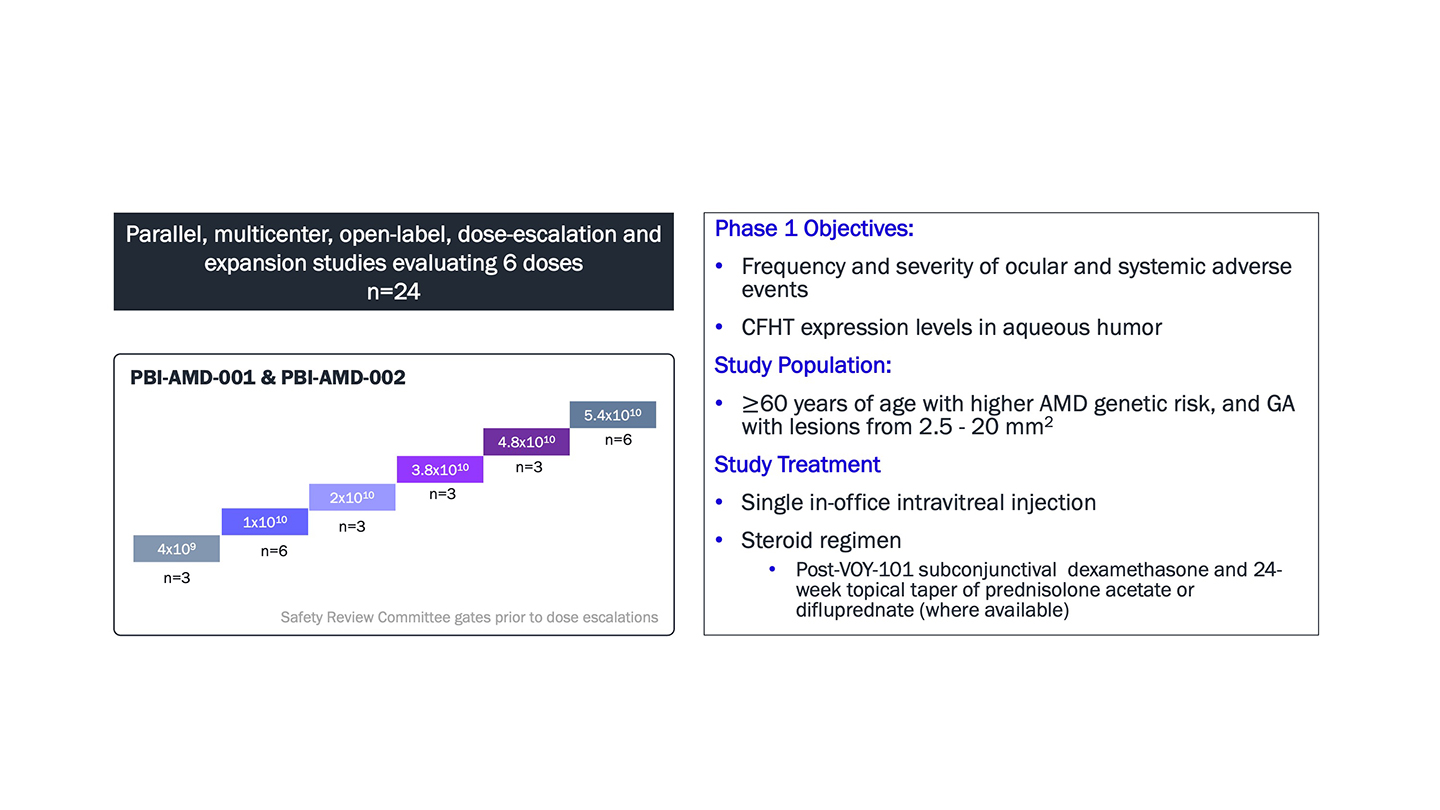
Figure 2. Design of the phase 1 PBI AMD-001 and PBI-AMD-002 trials of VOY-101 in GA.
Dr. Wykoff reported that no dose-limiting toxicities, treatment-related serious adverse events, vasculitis, retinitis, or study-eye choroidal neovascularization had been observed. Transient observations of mild cell represented the principal safety finding, occurring in 5 patients. “All of these events were first observed in months 1 or 2 after gene therapy dosing,” said Dr. Wykoff. “All of them were mild, transient, and controlled with topical steroids.” No flare or iris inflammation/abnormalities were observed. Importantly, Dr. Wykoff noted that no recurrences were observed after completion of the steroid taper. Three patients developed steroid-induced intraocular pressure (IOP) elevation, which was controlled with topical IOP-lowering medication.
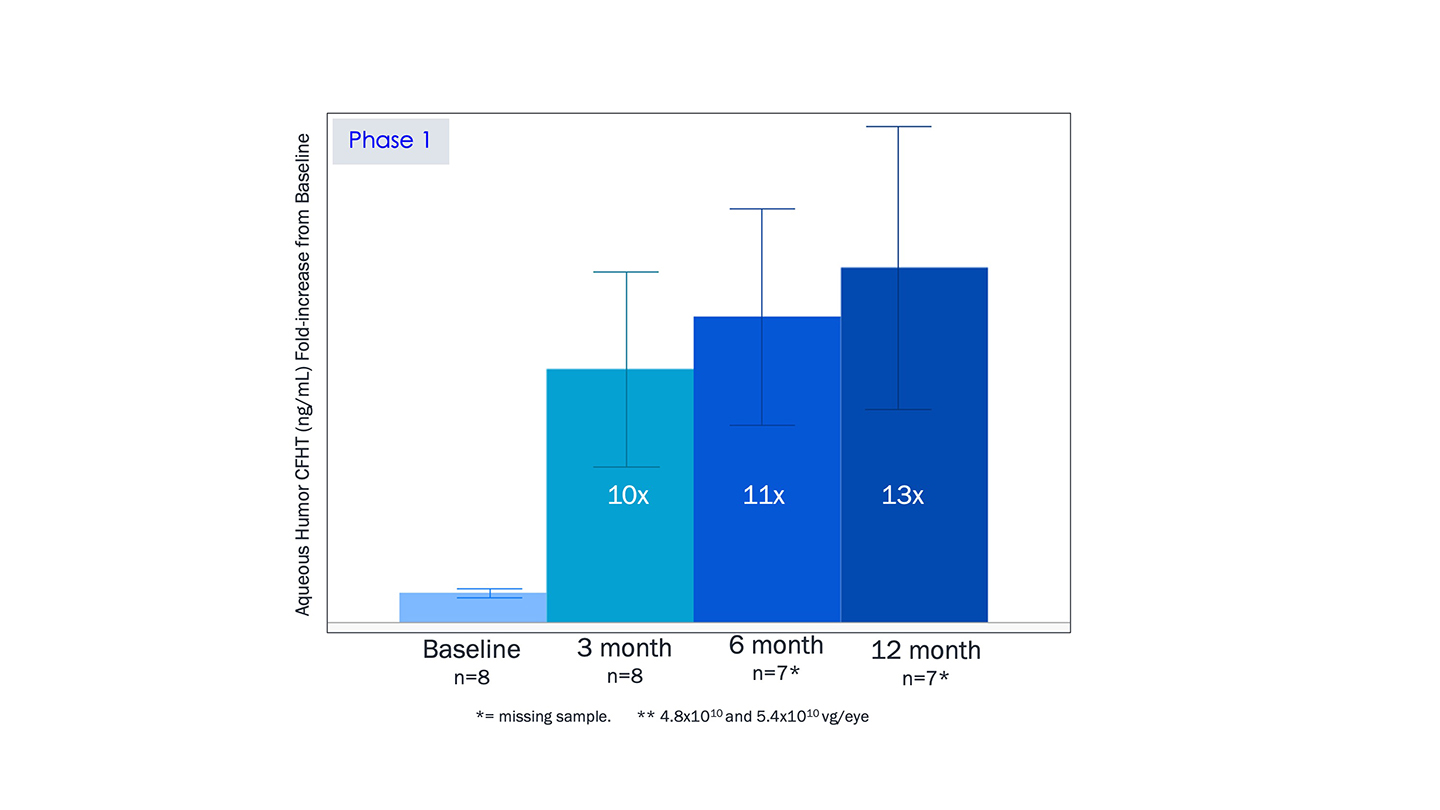
Figure 3. VOY-101 transgene expression in the 2 highest-dose cohorts are shown through months 3, 6, and 12 compared to baseline.
“Most important after safety is, of course, expression of the transgene,” noted Dr. Wykoff, who described how this was evaluated using aqueous humor CFHT levels. “We see consistent CFHT levels in aqueous humor among patients in the highest 2 dose cohorts after VOY-101 dosing from month 3 through 12, up to 13-fold above baseline (Figure 3).
The highest dose, 5.4×10^10 vector genomes [vg] per eye, was selected for further development in the phase 2 section of PBI-AMD-002, also called JOURNEY, which is currently enrolling (Figure 4). JOURNEY is a multicenter, open-label, fellow eye–controlled trial that plans to enroll 35 patients (70 eyes total). Participants are randomized so that 1 eye receives VOY-101 treatment while the fellow eye serves as the control. This fellow eye study design inherently controls for key variables in AMD including genetics, age and environmental exposures; in addition, eligibility criteria required reasonable GA size symmetry between the eyes to allow for comparison of progression. Phase 2 uses a prophylactic steroid regimen consisting of subconjunctival dexamethasone followed by a 6-month topical difluprednate taper; Difluprednate was selected due to its superior control of gene-therapy-related inflammation and significantly lower frequency of administration compared to prednisolone acetate. The primary endpoint is GA lesion growth at 15 months.

Figure 4. The phase 2a JOURNEY study uses a fellow-eye control design to reduce variability related to matched genetics, age, and environmental exposures while evaluating VOY-101 in geographic atrophy.
Preliminary phase 2 safety data with a mean follow up of 107 days was similar without vasculitis, retinitis, choroiditis, pigmentary changes or optic neuropathy. Study eye IOP increase associated with steroid use was the most commonly reported adverse event to date. Two 1-time observations of trace cell were reported and fully resolved.
VOY-101 was reported to be safe and well-tolerated with 13-fold expression of protective CFHT in phase 1 with 17/24 patients completing 24 month follow up to date, concluded Dr. Wykoff. These data, he said, support the potential for VOY-101 to be a one-time injection that can offer patients a well-tolerated, ongoing delivery of a protective form of complement protein that restores regulation of the complement cascade to treat GA without the need for monthly injections. RP