





What comes to mind when trainees hear the word uveitis? Ophthalmology residents often describe the field as “scary,” “hard,” or “bewildering,” alongside terms like “interesting,” “rewarding,” and even “fun.” When residents are asked why they do not seriously consider uveitis fellowship, the reasons certainly are not for a lack of opportunities for long-term longitudinal care of a diverse group of patients, fascinating pathology, and rewarding career. Instead, 3 common myths tend to dominate perceptions:
- There are few surgical opportunities in uveitis;
- Uveitis specialists are poorly compensated; and
- Uveitis is difficult to manage.
Drawing on new data from the American Uveitis Society (AUS) and insights from practicing uveitis specialists across the United States, these misconceptions can be addressed directly.
Myth 1: There Are Few Surgical Opportunities in Uveitis
This is perhaps the most pervasive misconception among trainees. In reality, uveitis is both a medical and surgical subspecialty. According to the 2025 AUS Member Practice Survey, more than 70% of uveitis specialists perform intravitreal injections or surgical procedures, including cataract extraction, glaucoma procedures, and, among dual-trained specialists, vitreoretinal surgery.1 Nearly 60% perform cataract surgery routinely, and more than 75% administer intravitreal injections as part of uveitis care.1
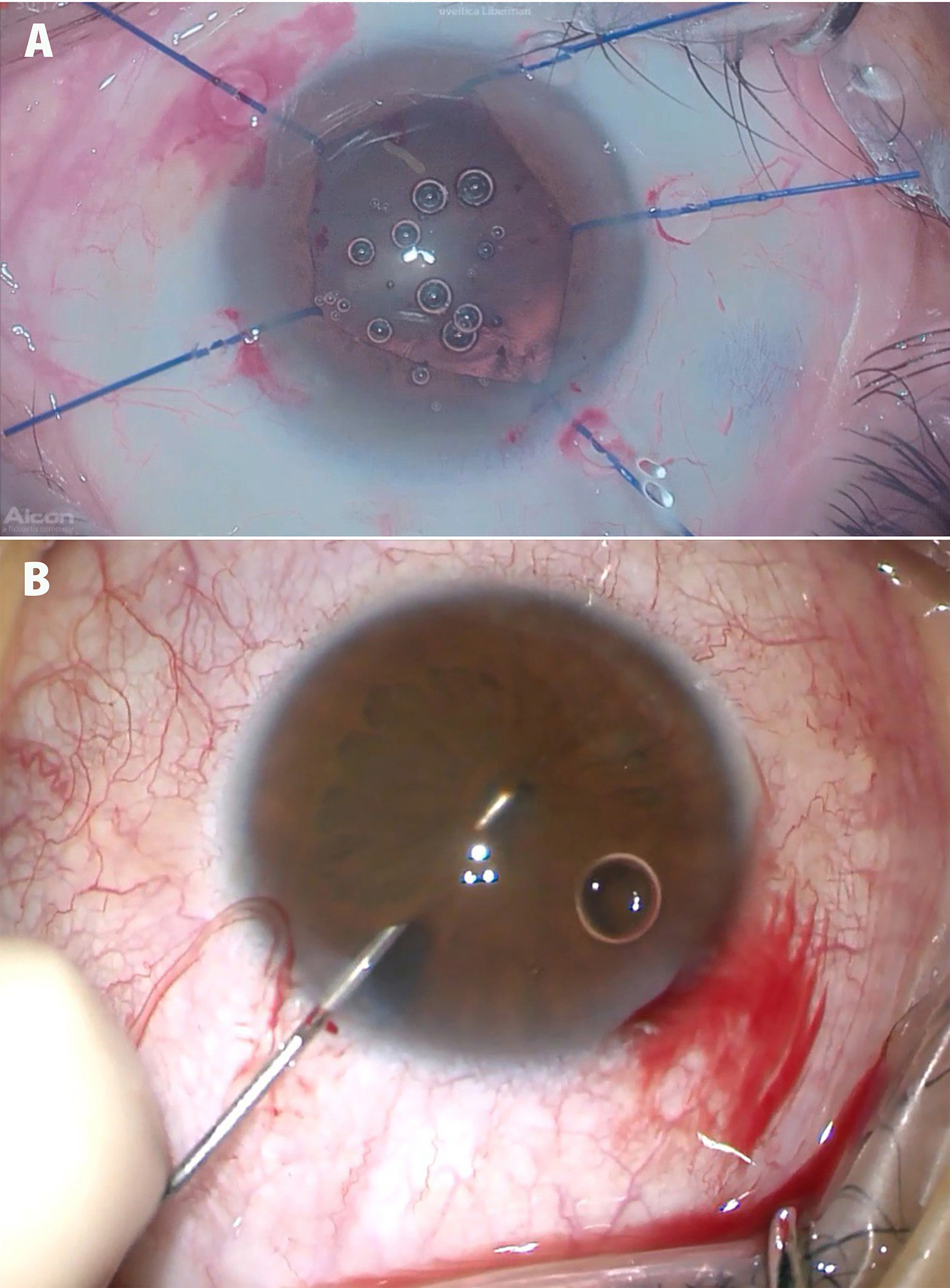
Figure 1. Uveitis specialists are often ideally situated to manage their patients’ cataracts, including perioperative (A) and intraoperative (B) management.
Uveitis specialists uniquely combine surgical expertise with nuanced perioperative management, including optimization of steroid timing, systemic immunomodulation, and antimicrobial coverage to reduce postoperative inflammation (Figure 1). Procedures such as anterior chamber paracentesis and vitreous tap for viral or atypical etiologies are far more common in uveitis practice than in general ophthalmology clinics.
As infectious anterior uveitis, particularly herpetic disease, becomes increasingly recognized, these procedural skills are in growing demand.2,3 Many uveitis specialists also maintain hybrid practices that include nonuveitic cataract or anterior segment surgery.4
Consider this myth busted! Uveitis can be as procedural and hands-on as the clinician desires and rewards those who enjoy diagnostic problem-solving and surgical care.
Myth 2: Uveitis Specialists Are Poorly Compensated
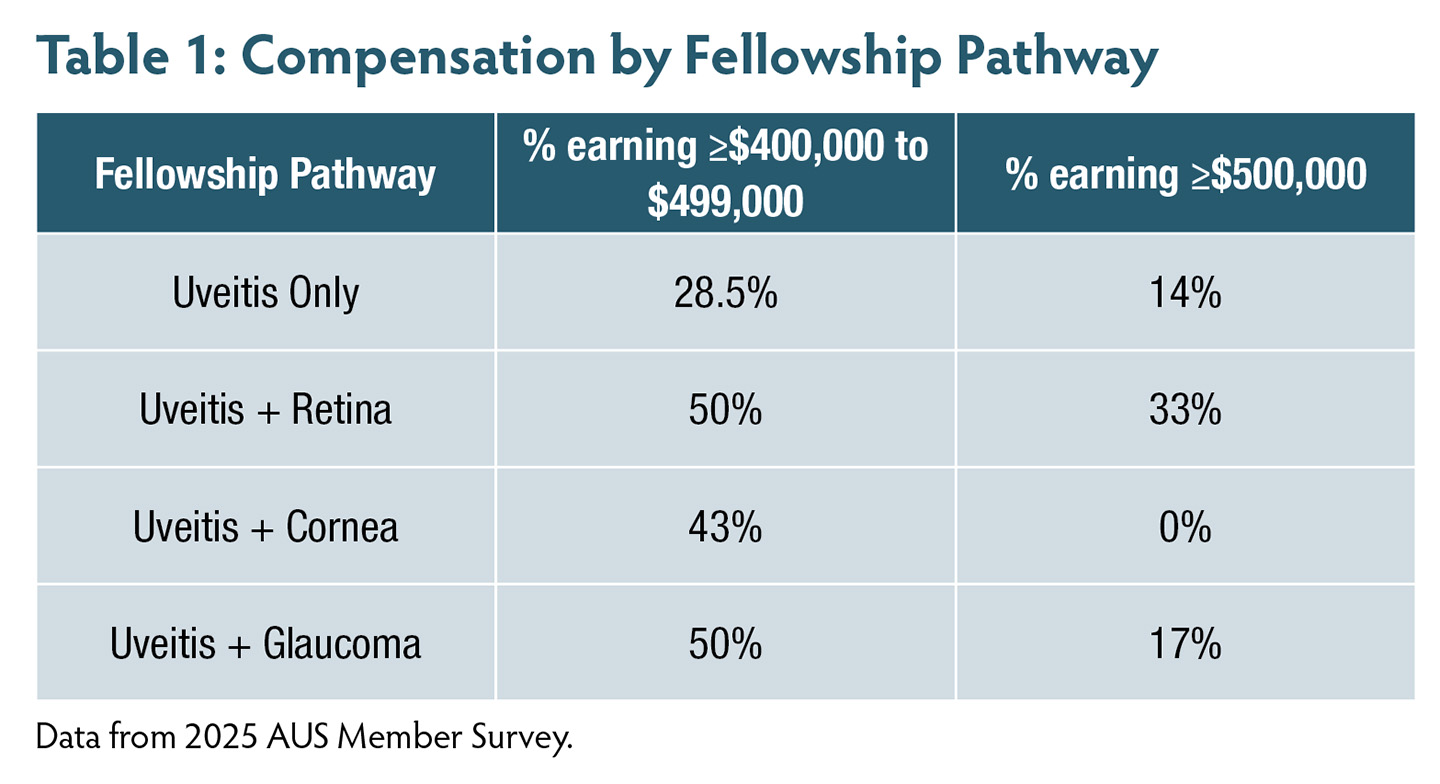
The perception of uveitis as a low-income career has persisted, even among some specialists. However, available data do not support this view. The 2025 AUS Member Survey found that most uveitis specialists report annual compensation between $300,000 and $400,000, with nearly 25% earning more than $400,000—figures comparable to other ophthalmic subspecialties.1 Specialists with additional fellowship training in retina, cornea, or glaucoma reported the highest compensation ranges, often exceeding $500,000 (Table 1).
It is true that uveitis care involves unique challenges: managing complex ocular disease, sometime in the setting of complex systemic conditions, reviewing immunologic labs, and coordinating care with rheumatology, infectious disease, or hematology colleagues. But these tasks are not burdens. Instead, they’re differentiators. They expand the physician’s reach and professional relationships, and they often translate to more stable, loyal referral bases. Moreover, academic uveitis specialists report some of the highest levels of professional satisfaction in ophthalmology, frequently citing “intellectual challenge” and “long-term patient impact” as key motivators.5
Another myth busted! Uveitis is not a low-paying field. It’s a field that rewards depth, collaboration, and expertise—often with compensation and lifestyle flexibility to match.
Myth 3: Uveitis Is Hard
A more accurate framing is that uveitis appears difficult when exposure and training are limited. Approximately half of US ophthalmology residents report no dedicated uveitis rotation, and most exposure occurs through textbook-based learning in the American Academy of Ophthalmology’s Basic and Clinical Science Course.5 This limited experience can foster the perception that uveitis is opaque or best managed outside ophthalmology.
That perception shifts with clinical exposure. Residents who rotate early with a uveitis specialist are twice as likely to consider fellowship training.5 Once they encounter the pattern recognition, diagnostic clarity, and often rapid visual improvement associated with uveitis care, initial hesitation frequently dissipates.
To address this exposure gap, the AUS Understanding Viewpoints and Expectations in Applicants (UVEA) Task Force has launched 2 initiatives aimed at making uveitis more approachable:
- A resident education portal, expected to launch in 2026, featuring triage guides, imaging modules, and “day-in-the-life” perspectives from practicing uveitis specialists; and
- A regional Champion Lecture Series connecting AUS faculty with residency programs lacking local uveitis mentorship.
For those pursuing formal training, 19 AUPO-accredited uveitis fellowship programs in the United States provide structured education in both medical and surgical management.
Myth busted! Uveitis is not inherently difficult; it is under-taught. With adequate exposure, it becomes one of the most intellectually and emotionally rewarding career paths in ophthalmology
Final Thoughts
Uveitis is not an esoteric niche in ophthalmology; it is a dynamic, multidisciplinary specialty at the intersection of surgery, immunology, and vision restoration. Its practitioners are defined not by a tolerance for complexity alone, but by precision, curiosity, and commitment to long-term patient outcomes. For residents seeking a field that challenges the intellect, values collaboration, and rewards innovation, uveitis might just be the best-kept secret in ophthalmology! RP





References
1. American Uveitis Society (AUS) Member Practice Survey, 2025.
2. Thorne JE, Skup M, Tundia N, et al. Direct and indirect resource use, healthcare costs, and workforce absence in patients with noninfectious intermediate, posterior, or panuveitis. Acta Ophthalmol. 2016;94(5):e345-353. doi:10.1111/aos.12987
3. Kump LI, Cervantes-Castaneda R, Androudi SN, Foster CS. Analysis of pediatric uveitis cases at a tertiary referral center. Ophthalmology. 2005;112(7):1287-1292. doi:10.1016/j.ophtha.2005.01.044
4. Tsui E, Crowell EL, Gangaputra S, et al. Current landscape of uveitis specialists in the United States. J Acad Ophthalmol. 2022;14(2):e187-e192. doi:10.1055/s-0042-1755581
5. Bosque L, Gonzales J, Kodati S, Berkenstock M. Understanding perception of ophthalmology residents on pursuing a uveitis fellowship. Curr J Ophthalmol. Manuscript submitted for publication 2026.