






Retinal vasoproliferative tumors (VPTs) are rare, acquired vascular lesions that can threaten vision if left untreated. Understanding their clinical presentation, differential diagnoses, and management strategies is essential for ophthalmologists, particularly when distinguishing VPTs from other retinal vascular tumors such as hemangioblastomas. Advances in imaging and treatment modalities have improved detection and visual outcomes, although challenges remain in peripheral lesion visualization and management of secondary cases associated with inflammation or degenerative retinal disease.
Introduction
Retinal vascular tumors may be congenital—such as retinal cavernous hemangioma and retinal arteriovenous communications (Wyburn-Mason syndrome)—or acquired, including retinal hemangioblastoma and VPTs.1 The distinction between congenital and acquired forms relates to the integrity of retinal tight junctions: congenital tumors generally have intact tight junctions and therefore lack subretinal fluid or lipid exudates, whereas acquired tumors involve disruption of these junctions, leading to vascular leakage with associated subretinal fluid or lipid exudation. Retinal VPTs and retinal hemangioblastoma are both acquired tumors, each with characteristic clinical features and specific systemic associations.
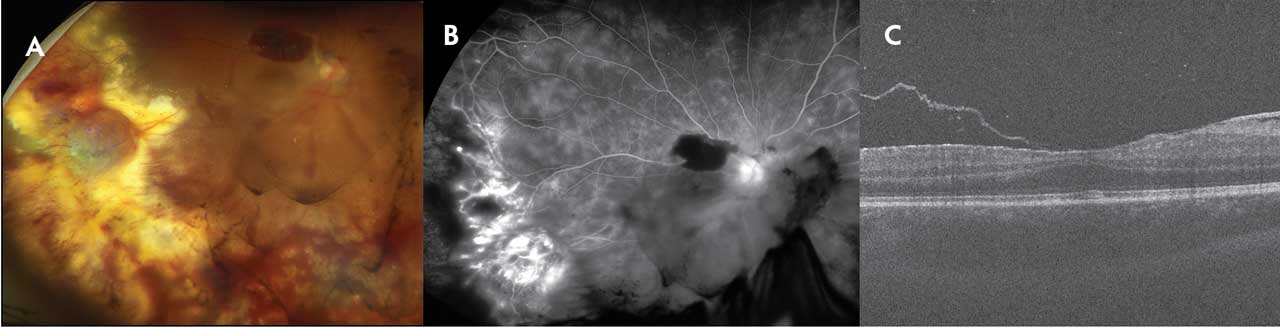
Figure 1. Typical features of retinal vasoproliferative tumor. Fundus photograph (A) showing prominent retinal lipid exudation, mild vitreous hemorrhage, and ill-defined retinal mass (8.0 x 6.0 x 2.3 mm in the inferotemporal periphery). Fluorescein angiogram (B) reveals adjacent areas of retinal capillary non perfusion and telangiectasia. Mild associated epiretinal membrane was present (C).
VPT was first recognized as a distinct clinical entity in 1982 when Baines reported the combination of peripheral telangiectatic nodules and posterior fibrocellular membranes.2 Initially labeled as “presumed acquired retinal hemangiomas,”³ VPT has become the most widely used terminology.4 Histologically, the lesion consists of a mixture of glial cells, retinal pigment epithelial cells, macrophages, foreign body giant cells, and a network of capillaries with some larger blood vessels.5-7 Tumor formation is considered reactive rather than neoplastic and is described as a retinal reactive astrocytic tumor.8 The underlying cause is often unidentified (primary, 87%), with inflammation (uveitis) or degenerative disease (retinitis pigmentosa) observed in secondary cases (13%).4
Clinical Features
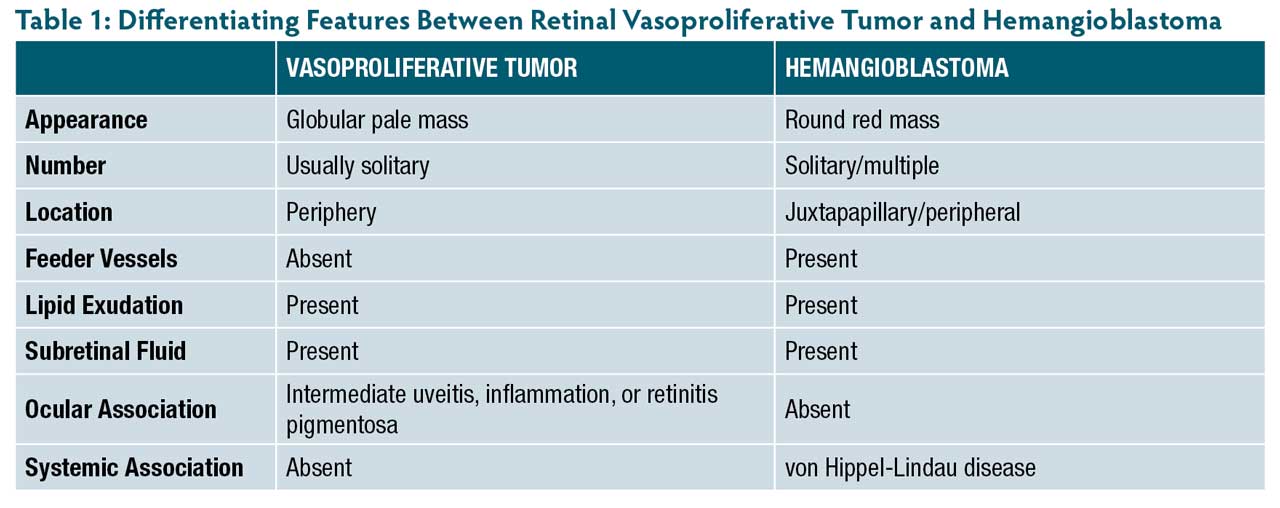
Primary VPTs are usually solitary, whereas secondary tumors tend to be multiple. Vasoproliferative tumors typically present in the third or fourth decade of life, with equal sex distribution.4 Secondary VPTs often occur at a younger age.9 Common presenting symptoms include reduced vision, photopsia, and metamorphopsia, although some cases are diagnosed incidentally. Clinically, VPT appears as a globular yellow-pink, vascular mass in the inferotemporal peripheral retina (Figure 1A). The lesion has direct communication with retinal vessels of normal caliber, in contrast to retinal hemangioblastomas, which exhibit dilated and tortuous feeder vessels. Salient differentiating features between VPT and hemangioblastoma are summarized in Table 1.10
Subretinal fluid, lipid exudation, hemorrhage, and gliosis may obscure the tumor. Associated macular fibrosis and edema can lead to visual loss. Peripheral location complicates imaging with fluorescein angiography, ultrasonography, and optical coherence tomography (OCT). On fluorescein angiography, VPT demonstrates early hyperfluorescence with increasing diffuse leakage in late phases (Figure 1B). Telangiectatic and microaneurysmal changes, as well as capillary dropout reminiscent of Coats disease, may be observed in surrounding areas.1
Treatment
Management depends on tumor size and activity.1 Small, asymptomatic, gliotic tumors may be observed periodically. Treatment is indicated if the lesion is “active,” defined by the presence of subretinal fluid, hemorrhage, or lipid exudation. Tumors ≤1.5 mm can be treated with laser photocoagulation applied directly to the tumor, surrounding retina, and feeder vessels. Slightly larger tumors (up to 4.5 mm) are best treated with transconjunctival cryotherapy using a triple freeze-thaw cycle. Large tumors with ill-defined margins due to extensive exudation are technically challenging to treat with cryotherapy; these are better managed with radiation therapy, including plaque brachytherapy (ruthenium or iodine)11,12 or CyberKnife stereotactic radiotherapy (Accuray).13,14 Sequelae such as radiation retinopathy manifesting as cystoid macular edema or retinal neovascularization should be anticipated. Posteriorly located tumors with well-defined margins are best managed with photodynamic therapy (Figure 1C).15-17
Intravitreal anti-VEGF therapy and dexamethasone implants (Ozurdex; AbbVie) may be used adjunctively with cryotherapy, photodynamic therapy, or radiation therapy to prevent macular edema.18,19 In secondary VPT associated with uveitis, concomitant control of inflammation is necessary.20
Prognosis
Even small VPTs can cause significant vision loss, emphasizing the need for timely management.1 Advanced cases may progress to neovascular glaucoma, occasionally necessitating enucleation. Secondary VPTs tend to have worse visual outcomes.9 RP


References
1. Salvi SM, Bouhout S, Singh AD. Retinal vascular tumors. In: Singh AD, Damato BE, eds. Clinical Ophthalmic Oncology: Retinal Tumors. Cham, Switzerland: Springer Nature; 2024.
2. Baines PS, Hiscott PS, McLeod D. Posterior non-vascularized proliferative extraretinopathy and peripheral nodular retinal telangiectasis. Trans Ophthalmol Soc UK. 1982;102(Pt 4):487-491.
3. Shields JA, Decker WL, Sanborn GE, Augsburger JJ, Goldberg RE. Presumed acquired retinal hemangiomas. Ophthalmology. 1983;90(11):1292-1300. doi:10.1016/s0161-6420(83)34389-x
4. Shields CL, Shields JA, Barrett J, De Potter P. Vasoproliferative tumors of the ocular fundus. Classification and clinical manifestations in 103 patients. Arch Ophthalmol. 1995;113(5):615-623. doi:10.1001/archopht.1995.01100050083035
5. Hiscott P, Mudhar H. Is vasoproliferative tumour (reactive retinal glioangiosis) part of the spectrum of proliferative vitreoretinopathy? Eye (Lond). 2009;23(9):1851-1858. doi:10.1038/eye.2008.351
6. Irvine F, O’Donnell N, Kemp E, Lee WR. Retinal vasoproliferative tumors: surgical management and histological findings. Arch Ophthalmol. 2000;118(4):563-569. doi:10.1001/archopht.118.4.563
7. Singh AD, Soto H, Bellerive C, Biscotti CV. Reactive retinal astrocytic tumor (focal nodular gliosis): report of the clinical spectrum of 3 cases. Ocul Oncol Pathol. 2017;3(3):235-239. doi:10.1159/000455151
8. Grossniklaus HE, Lenis TL, Jakobiec FA. Retinal reactive astrocytic tumor (focal nodular gliosis): the entity also known as vasoproliferative tumor. Ocul Oncol Pathol. 2017;3(3):161-163. doi:10.1159/000455149
9. Shields CL, Kaliki S, Al-Dahmash S, et al. Retinal vasoproliferative tumors: comparative clinical features of primary vs secondary tumors in 334 cases. JAMA Ophthalmol. 2013;131(3):328-334. doi:10.1001/jamaophthalmol.2013.1844
10. Singh AD, Shields CL, Shields JA. von Hippel-Lindau disease. Surv Ophthalmol. 2001;46(2):117-142. doi:10.1016/S0039-6257(00)00156-0
11. Cohen VML, Shields CL, Demirci H, Shields JA. Iodine I 125 plaque radiotherapy for vasoproliferative tumors of the retina in 30 eyes. Arch Ophthalmol. 2008;126(9):1245-1251. doi:10.1001/archopht.126.9.1245
12. Anastassiou G, Bornfeld N, Schueler AO, et al. Ruthenium-106 plaque brachytherapy for symptomatic vasoproliferative tumours of the retina. Br J Ophthalmol. 2006;90(4):447-450. doi:10.1136/bjo.2005.085723
13. Ipek SC, Tunc M, Oysul K, et al. CyberKnife stereotactic radiotherapy in secondary vasoproliferative tumor of the retina. Case Rep Ophthalmol. 2021;12(1):264-269. doi:10.1159/000511022
14. Schmelter V, Fuerweger C, Muacevic A, et al. Robotic-assisted radiosurgery for the treatment of vasoproliferative tumours. Acta Ophthalmol. 2021;99(4):456-460. doi:10.1111/aos.14579
15. Barbezetto IA, Smith RT. Vasoproliferative tumor of the retina treated with photodynamic therapy. Retina. 2003;23(4):565-567. doi:10.1097/01.iae.0000078771.69757.8b
16. Bertelli E, Pernter H. Vasoproliferative retinal tumor treated with indocyanine green-mediated photothrombosis. Retin Cases Brief Rep. 2009;3(3):266-271. doi:10.1097/ICB.0b013e3181737700
17. Saldanha MJ, Edrich C. Treatment of vasoproliferative tumors with photodynamic therapy. Ophthalmic Surg Lasers Imaging. 2008;39(2):143-145. doi:10.3928/15428877-20080301-13
18. Kenawy N, Groenwald C, Damato B. Treatment of a vasoproliferative tumour with intravitreal bevacizumab (Avastin). Eye (Lond). 2007;21(6):893-894. doi:10.1038/sj.eye.6702782
19. Cebeci Z, Oray M, Tuncer S, et al. Intravitreal dexamethasone implant (Ozurdex) and photodynamic therapy for vasoproliferative retinal tumours. Can J Ophthalmol. 2014;49(4):e83-e84. doi:10.1016/j.jcjo.2014.04.006
20. Pichi F, Neri P, Agarwal A, et al. Vasoproliferative tumors in intermediate uveitis. Retina. 2020;40(9):1765-1773. doi:10.1097/IAE.0000000000002656